Disease Elimination Program, Burnet Institute, Melbourne, Australia; Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Victoria, Australia.
Disease Elimination Program, Burnet Institute, Melbourne, Australia; Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; School of Population and Global Health, The University of Melbourne, Parkville, Australia.
Epidemics. 2023 Sep;44:100702. doi: 10.1016/j.epidem.2023.100702. Epub 2023 Jun 14.
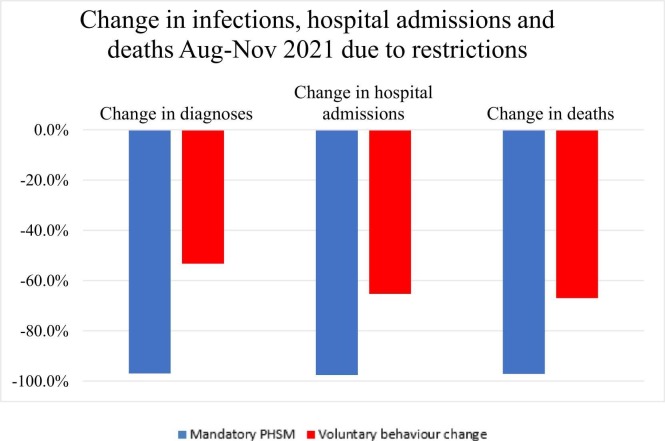
Prior to mid-2021, Australia's approach to COVID-19 was to eliminate community transmission. However, between August-November 2021, the state of Victoria, Australia, experienced an outbreak of the Delta variant that continued to grow despite extensive lockdowns and public health measures in place. While these public health restrictions were ultimately unable to stop community transmission, they likely had a major impact reducing transmission and adverse health outcomes relative to voluntary risk-mitigation only (e.g., in response to rising cases and deaths, some people may avoid crowded settings, hospitality, retail, social occasions, or indoor settings). This study aims to estimate the impact of the August-November 2021 enforced public health restrictions in Victoria, compared to voluntary risk-mitigation only.
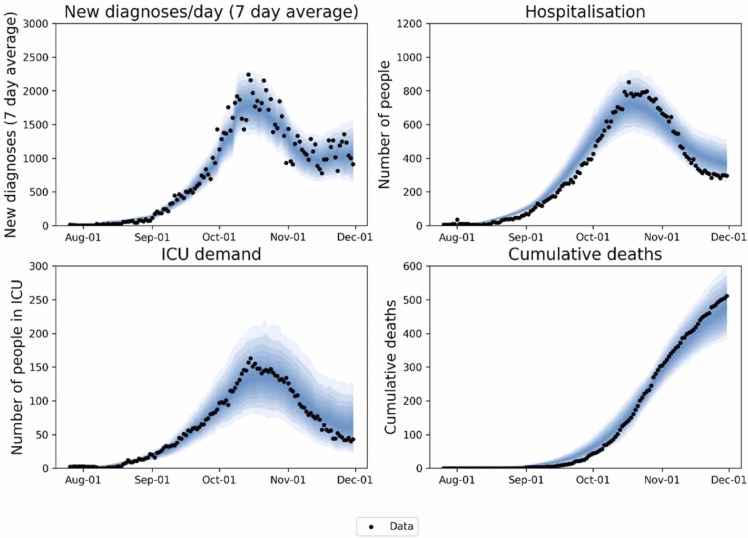
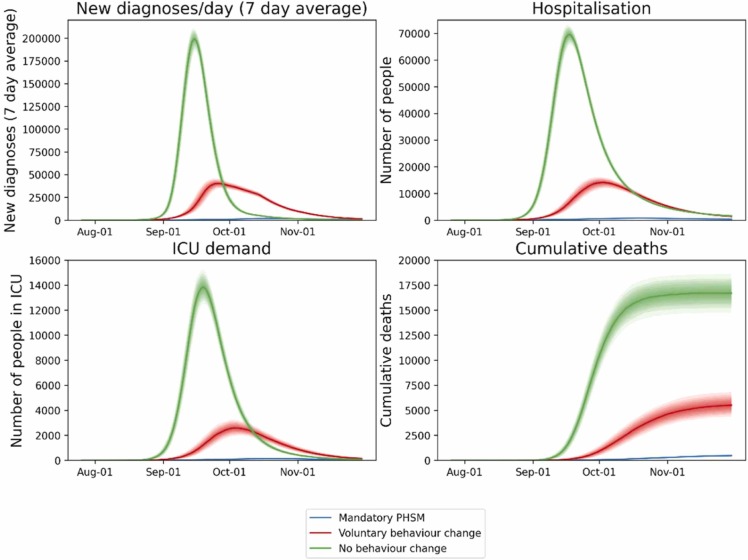
An agent-based model was calibrated to Victorian epidemiological, health and behavioural data from 1 August to 30 November 2021, as well as policies that were implemented over that period. Two counter-factual scenarios were run for the same period with (a) no restrictions in place; or (b) voluntary risk-mitigation only, based on behaviour measured over the December-January Omicron BA.1 epidemic wave when restrictions were not in place.
Over August-November 2021, the baseline model scenario resulted in 97,000 (91,000-102,000) diagnoses, 9100 (8500-9700) hospital admissions, and 480 (430-530) deaths. Without any restrictions in place, there were 3,228,000 (3,200,000-3,253,000) diagnoses, 375,100 (370,200-380,900) hospital admissions, and 16,700 (16,000-17,500) deaths. With voluntary risk-mitigation equal to those observed during the Omicron BA.1 epidemic wave, there were 1,507,000 (1,469,000-1,549,000) diagnoses, 130,300 (124,500-136,000) hospital admissions, and 5500 (5000-6100) deaths.
Public health restrictions implemented in Victoria over August-November 2021 are likely to have averted more than 120,000 hospitalizations and 5000 deaths relative to voluntary risk-mitigation only. During a COVID-19 epidemic wave voluntary behaviour change can reduce transmission substantially, but not to the same extent as enforced restrictions.
在 2021 年年中之前,澳大利亚采取的方法是消除社区传播。然而,在 2021 年 8 月至 11 月期间,澳大利亚维多利亚州爆发了 Delta 变体疫情,尽管采取了广泛的封锁和公共卫生措施,但疫情仍在持续蔓延。虽然这些公共卫生限制最终未能阻止社区传播,但与仅自愿采取风险缓解措施相比,它们可能对减少传播和不良健康结果产生了重大影响(例如,为了应对病例和死亡人数的增加,有些人可能会避免拥挤的场所、餐饮、零售、社交场合或室内场所)。本研究旨在估计 2021 年 8 月至 11 月在维多利亚州实施的强制性公共卫生限制措施与仅自愿采取风险缓解措施相比的影响。
根据 2021 年 8 月 1 日至 11 月 30 日维多利亚州的流行病学、健康和行为数据以及在此期间实施的政策,对基于主体的模型进行了校准。在同一时期,针对两种反事实情景进行了模拟:(a)不实施任何限制;或(b)仅根据 2021 年 12 月至 1 月期间 Omicron BA.1 疫情期间未实施限制时测量的行为,实施自愿风险缓解措施。
在 2021 年 8 月至 11 月期间,基线模型情景导致 97000 例(91000-102000)诊断、9100 例(8500-9700)住院和 480 例(430-530)死亡。如果不实施任何限制,将有 3228000 例(3200000-3253000)诊断、375100 例(3702000-3809000)住院和 16700 例(16000-17500)死亡。在 Omicron BA.1 疫情期间实施与观察到的自愿风险缓解措施相等的措施时,将有 1507000 例(1469000-1549000)诊断、130300 例(124500-136000)住院和 5500 例(5000-6100)死亡。
与仅自愿采取风险缓解措施相比,2021 年 8 月至 11 月在维多利亚州实施的公共卫生限制措施可能避免了超过 120000 例住院和 5000 例死亡。在 COVID-19 疫情期间,自愿改变行为可以大大减少传播,但不如强制限制有效。