SHARE Collaborative, Department of Immunobiology, Queen Mary University of London, London, United Kingdom.
National Hemophilia Center, Sheba Medical Center, Ramat Gan, Israel.
Clin Infect Dis. 2023 Nov 17;77(10):1423-1431. doi: 10.1093/cid/ciad370.
Previously reported post hoc multivariable analyses exploring predictors of confirmed virologic failure (CVF) with cabotegravir + rilpivirine long-acting (CAB + RPV LA) were expanded to include data beyond week 48, additional covariates, and additional participants.
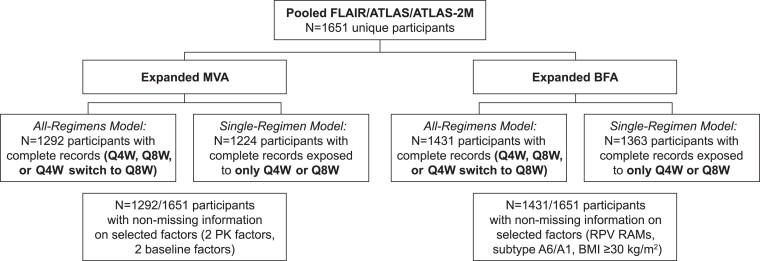
Pooled data from 1651 participants were used to explore dosing regimen (every 4 or every 8 weeks), demographic, viral, and pharmacokinetic covariates as potential predictors of CVF. Prior dosing regimen experience was accounted for using 2 populations. Two models were conducted in each population-baseline factor analyses exploring factors known at baseline and multivariable analyses exploring baseline factors plus postbaseline model-predicted CAB/RPV trough concentrations (4 and 44 weeks postinjection). Retained factors were evaluated to understand their contribution to CVF (alone or in combination).
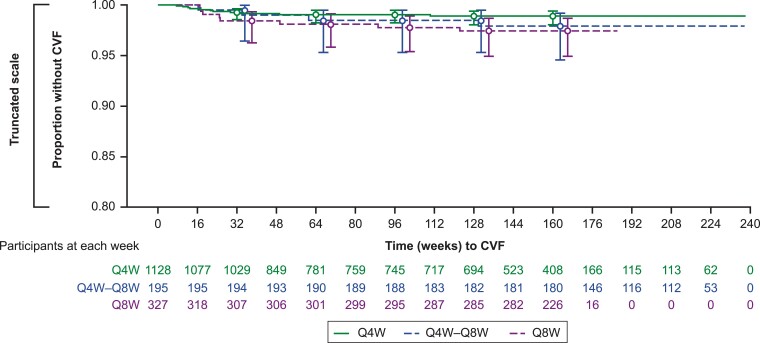
Overall, 1.4% (n = 23/1651) of participants had CVF through 152 weeks. The presence of RPV resistance-associated mutations, human immunodeficiency virus-1 subtype A6/A1, and body mass index ≥30 kg/m2 were associated with an increased risk of CVF (P < .05 adjusted incidence rate ratio), with participants with ≥2 of these baseline factors having a higher risk of CVF. Lower model-predicted CAB/RPV troughs were additional factors retained for multivariable analyses.
The presence of ≥2 baseline factors (RPV resistance-associated mutations, A6/A1 subtype, and/or body mass index ≥30 kg/m2) was associated with increased CVF risk, consistent with prior analyses. Inclusion of initial model-predicted CAB/RPV trough concentrations (≤first quartile) did not improve the prediction of CVF beyond the presence of a combination of ≥2 baseline factors, reinforcing the clinical utility of the baseline factors in the appropriate use of CAB + RPV LA.
此前报道的事后多变量分析探索了卡替拉韦/利匹韦林长效(CAB/RPV LA)治疗中确认病毒学失败(CVF)的预测因素,这些分析扩展到包括第 48 周以后的数据、其他协变量和更多参与者。
使用来自 1651 名参与者的汇总数据,探索了剂量方案(每 4 周或每 8 周)、人口统计学、病毒学和药代动力学协变量作为 CVF 的潜在预测因素。既往剂量方案经验使用 2 个人群来考虑。在每个人群中进行了 2 种模型——基于基线的因素分析,探索了基线时已知的因素,以及多变量分析,探索了基线因素加注射后 4 和 44 周时预测的 CAB/RPV 谷浓度。保留的因素进行了评估,以了解它们对 CVF 的贡献(单独或组合)。
总体而言,1651 名参与者中有 1.4%(n=23)在 152 周时发生 CVF。存在 RPV 耐药相关突变、人类免疫缺陷病毒-1 亚型 A6/A1 和体重指数≥30 kg/m2 与 CVF 风险增加相关(P<0.05 调整后的发生率比),具有≥2 个这些基线因素的参与者 CVF 风险更高。较低的预测模型 CAB/RPV 谷浓度是多变量分析中保留的其他因素。
≥2 个基线因素(RPV 耐药相关突变、A6/A1 亚型和/或体重指数≥30 kg/m2)的存在与 CVF 风险增加相关,与之前的分析一致。纳入初始预测模型 CAB/RPV 谷浓度(≤第一四分位数)并不能提高 CVF 的预测效果,除了≥2 个基线因素的组合外,这强化了基线因素在 CAB/RPV LA 正确使用中的临床实用性。