Cichocka-Jarosz Ewa, Brzyski Piotr, Jedynak-Wąsowicz Urszula, Mól Nina, Klasa Barbara, Mazurek-Durlak Zofia, Lis Grzegorz, Nowak-Węgrzyn Anna
Department of Paediatrics, Jagiellonian University Medical College, 265 Wielicka St, 30-663 Krakow, Poland.
Dziupla",Statistical Analysis, Warszawa, Poland.
World Allergy Organ J. 2023 May 10;16(5):100775. doi: 10.1016/j.waojou.2023.100775. eCollection 2023 May.
The basis for qualification for venom immunotherapy (VIT) is the fulfilment of both the clinical and immunological criteria. Diagnostic tests that confirm the immunological criterion of an IgE-mediated sensitization include skin prick tests (SPT), intradermal tests (IDT), and serum specific IgE (sIgE) for the culprit venom.
This study aimed to assess the usefulness of SPT as the immunological marker in the diagnosis of insect venom sensitization in children with history of systemic reaction (SR) to insect sting evaluated by means of I-IV-grades Mueller's scale. There are no such studies in children.
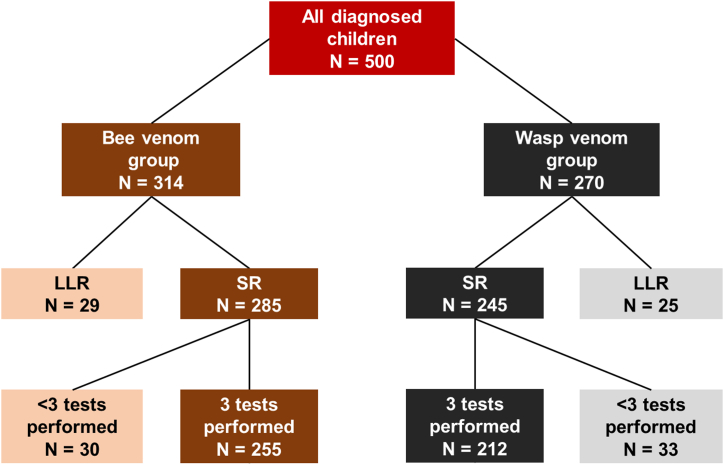
This cross-sectional study sample consisted of 416 children aged 3-18 years (mean age 10.6 ± 3.8), 76% males, all with the history of a systemic reaction (SR) after a Hymenoptera sting (48% of grade III/IV according to Mueller scale), diagnosed between 1999 and 2019 in the tertiary referral centre. The standard diagnostic tests were used. Specificity, sensitivity, and positive and negative predictive values were computed to assess the diagnostic properties of the clinical tests to distinguish between mild and severe SR. To assess the relative value of an individual test in predicting the qualification to VIT we incorporated the Shapley value (SV).
Positive SPT results were found in up to no more than 3% of children; among them less than 1% had only positive SPT and were negative for sIgE and IDT. Approximately 85% of the children had detectable venom sIgE, followed by positive IDT (75%). Almost 70% of children had positive both sIgE and IDT results. In children with grade III/IV reaction, about 80% of children had positive results of both of these tests. sIgE and IDT had sensitivity >0.80, whereas SPT had high specificity (>0.97) in differentiating between mild and severe SR. Relative value of diagnostic tests in predicting qualification to VIT varied between venoms. Bee venom IDT had higher SV (0.052) than sIgE (0.041). In contrast, wasp venom sIgE had higher SV (0.075) than IDT (0.035).
SPTs are not an useful immunological marker of venom sensitization in children, and eliminating SPT does not result in a loss of diagnostic accuracy. Limiting diagnostics to venom sIgE and IDT would shorten the procedure and reduce costs. Future studies are needed to determine if venom sIgE as the first line diagnostic test, with IDT added only if the venom sIgE is undetectable, is an optimal diagnostic process.
毒液免疫疗法(VIT)的资格认定依据是同时满足临床和免疫学标准。确认IgE介导的致敏反应免疫学标准的诊断测试包括皮肤点刺试验(SPT)、皮内试验(IDT)以及针对致病毒液的血清特异性IgE(sIgE)检测。
本研究旨在评估SPT作为免疫学标志物在诊断有昆虫叮咬全身反应(SR)病史儿童昆虫毒液致敏中的作用,这些儿童的SR严重程度通过I-IV级穆勒量表进行评估。此前尚无针对儿童的此类研究。
本横断面研究样本包括416名3至18岁儿童(平均年龄10.6±3.8岁),男性占76%,均有膜翅目昆虫叮咬后的全身反应(SR)病史(根据穆勒量表,48%为III/IV级),于1999年至2019年在三级转诊中心确诊。采用标准诊断测试。计算特异性、敏感性以及阳性和阴性预测值,以评估区分轻度和重度SR的临床测试的诊断性能。为评估个体测试在预测VIT资格方面的相对价值,我们纳入了沙普利值(SV)。
SPT结果呈阳性的儿童比例最高不超过3%;其中只有不到1%的儿童SPT呈阳性,而sIgE和IDT为阴性。约85%的儿童可检测到毒液sIgE,其次是IDT呈阳性(75%)。近70%的儿童sIgE和IDT结果均为阳性。在III/IV级反应的儿童中,约80%的儿童这两项测试结果均为阳性。sIgE和IDT在区分轻度和重度SR方面的敏感性>0.80,而SPT具有较高的特异性(>0.97)。不同毒液的诊断测试在预测VIT资格方面的相对价值有所不同。蜜蜂毒液IDT的SV(0.052)高于sIgE(0.041)。相比之下,黄蜂毒液sIgE的SV(0.075)高于IDT(0.035)。
SPT并非儿童毒液致敏的有用免疫学标志物,去除SPT不会导致诊断准确性的丧失。将诊断限制在毒液sIgE和IDT上可缩短流程并降低成本。未来需要开展研究以确定毒液sIgE作为一线诊断测试,仅在无法检测到毒液sIgE时才增加IDT,是否为最佳诊断流程。