Ruëff Franziska, Bauer Andrea, Becker Sven, Brehler Randolf, Brockow Knut, Chaker Adam M, Darsow Ulf, Fischer Jörg, Fuchs Thomas, Gerstlauer Michael, Gernert Sunhild, Hamelmann Eckard, Hötzenecker Wolfram, Klimek Ludger, Lange Lars, Merk Hans, Mülleneisen Norbert K, Neustädter Irena, Pfützner Wolfgang, Sieber Wolfgang, Sitter Helmut, Skudlik Christoph, Treudler Regina, Wedi Bettina, Wöhrl Stefan, Worm Margitta, Jakob Thilo
Department of Dermatology and Allergy, LMU University Hospital, Munich.
Department of Dermatology, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden.
Allergol Select. 2023 Oct 2;7:154-190. doi: 10.5414/ALX02430E. eCollection 2023.
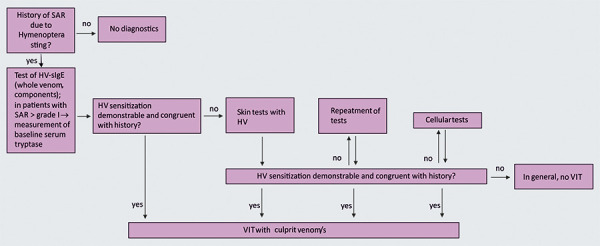
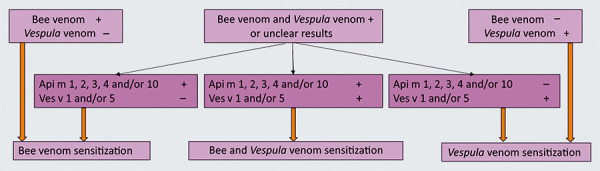
Hymenoptera venom (HV) is injected into the skin during a sting by Hymenoptera such as bees or wasps. Some components of HV are potential allergens and can cause large local and/or systemic allergic reactions (SAR) in sensitized individuals. During their lifetime, ~ 3% of the general population will develop SAR following a Hymenoptera sting. This guideline presents the diagnostic and therapeutic approach to SAR following Hymenoptera stings. Symptomatic therapy is usually required after a severe local reaction, but specific diagnosis or allergen immunotherapy (AIT) with HV (VIT) is not necessary. When taking a patient's medical history after SAR, clinicians should discuss possible risk factors for more frequent stings and more severe anaphylactic reactions. The most important risk factors for more severe SAR are mast cell disease and, especially in children, uncontrolled asthma. Therefore, if the SAR extends beyond the skin (according to the Ring and Messmer classification: grade > I), the baseline serum tryptase concentration shall be measured and the skin shall be examined for possible mastocytosis. The medical history should also include questions specific to asthma symptoms. To demonstrate sensitization to HV, allergists shall determine concentrations of specific IgE antibodies (sIgE) to bee and/or vespid venoms, their constituents and other venoms as appropriate. If the results are negative less than 2 weeks after the sting, the tests shall be repeated (at least 4 - 6 weeks after the sting). If only sIgE to the total venom extracts have been determined, if there is double sensitization, or if the results are implausible, allergists shall determine sIgE to the different venom components. Skin testing may be omitted if in-vitro methods have provided a definitive diagnosis. If neither laboratory diagnosis nor skin testing has led to conclusive results, additional cellular testing can be performed. Therapy for HV allergy includes prophylaxis of reexposure, patient self treatment measures (including use of rescue medication) in the event of re-stings, and VIT. Following a grade I SAR and in the absence of other risk factors for repeated sting exposure or more severe anaphylaxis, it is not necessary to prescribe an adrenaline auto-injector (AAI) or to administer VIT. Under certain conditions, VIT can be administered even in the presence of previous grade I anaphylaxis, e.g., if there are additional risk factors or if quality of life would be reduced without VIT. Physicians should be aware of the contraindications to VIT, although they can be overridden in justified individual cases after weighing benefits and risks. The use of β-blockers and ACE inhibitors is not a contraindication to VIT. Patients should be informed about possible interactions. For VIT, the venom extract shall be used that, according to the patient's history and the results of the allergy diagnostics, was the trigger of the disease. If, in the case of double sensitization and an unclear history regarding the trigger, it is not possible to determine the culprit venom even with additional diagnostic procedures, VIT shall be performed with both venom extracts. The standard maintenance dose of VIT is 100 µg HV. In adult patients with bee venom allergy and an increased risk of sting exposure or particularly severe anaphylaxis, a maintenance dose of 200 µg can be considered from the start of VIT. Administration of a non-sedating H1-blocking antihistamine can be considered to reduce side effects. The maintenance dose should be given at 4-weekly intervals during the first year and, following the manufacturer's instructions, every 5 - 6 weeks from the second year, depending on the preparation used; if a depot preparation is used, the interval can be extended to 8 weeks from the third year onwards. If significant recurrent systemic reactions occur during VIT, clinicians shall identify and as possible eliminate co-factors that promote these reactions. If this is not possible or if there are no such co-factors, if prophylactic administration of an H1-blocking antihistamine is not effective, and if a higher dose of VIT has not led to tolerability of VIT, physicians should should consider additional treatment with an anti IgE antibody such as omalizumab as off lable use. For practical reasons, only a small number of patients are able to undergo sting challenge tests to check the success of the therapy, which requires in-hospital monitoring and emergency standby. To perform such a provocation test, patients must have tolerated VIT at the planned maintenance dose. In the event of treatment failure while on treatment with an ACE inhibitor, physicians should consider discontinuing the ACE inhibitor. In the absence of tolerance induction, physicians shall increase the maintenance dose (200 µg to a maximum of 400 µg in adults, maximum of 200 µg HV in children). If increasing the maintenance dose does not provide adequate protection and there are risk factors for a severe anaphylactic reaction, physicians should consider a co-medication based on an anti-IgE antibody (omalizumab; off-label use) during the insect flight season. In patients without specific risk factors, VIT can be discontinued after 3 - 5 years if maintenance therapy has been tolerated without recurrent anaphylactic events. Prolonged or permanent VIT can be considered in patients with mastocytosis, a history of cardiovascular or respiratory arrest due to Hymenoptera sting (severity grade IV), or other specific constellations associated with an increased individual risk of recurrent and/or severe SAR (e.g., hereditary α-tryptasemia). In cases of strongly increased, unavoidable insect exposure, adults may receive VIT until the end of intense contact. The prescription of an AAI can be omitted in patients with a history of SAR grade I and II when the maintenance dose of VIT has been reached and tolerated, provided that there are no additional risk factors. The same holds true once the VIT has been terminated after the regular treatment period. Patients with a history of SAR grade ≥ III reaction, or grade II reaction combined with additional factors that increase the risk of non response or repeated severe sting reactions, should carry an emergency kit, including an AAI, during VIT and after regular termination of the VIT.
膜翅目昆虫毒液(HV)在蜜蜂或黄蜂等膜翅目昆虫蜇刺时注入皮肤。HV的某些成分是潜在的过敏原,可在致敏个体中引起严重的局部和/或全身过敏反应(SAR)。在其一生中,约3%的普通人群在被膜翅目昆虫蜇刺后会发生SAR。本指南介绍了膜翅目昆虫蜇刺后SAR的诊断和治疗方法。严重局部反应后通常需要对症治疗,但无需进行特异性诊断或HV过敏原免疫疗法(AIT)(VIT)。在SAR后采集患者病史时,临床医生应讨论更频繁蜇刺和更严重过敏反应的可能危险因素。更严重SAR的最重要危险因素是肥大细胞疾病,尤其是在儿童中,还有未控制的哮喘。因此,如果SAR超出皮肤范围(根据Ring和Messmer分类:分级> I),应测量基线血清类胰蛋白酶浓度,并检查皮肤是否可能存在肥大细胞增多症。病史还应包括针对哮喘症状的特定问题。为证明对HV过敏,过敏症专科医生应酌情测定针对蜜蜂和/或黄蜂毒液、其成分及其他毒液的特异性IgE抗体(sIgE)浓度。如果蜇刺后不到2周结果为阴性,应重复检测(至少在蜇刺后4 - 6周)。如果仅测定了针对总毒液提取物的sIgE,存在双重致敏,或结果不可信,过敏症专科医生应测定针对不同毒液成分的sIgE。如果体外方法已提供明确诊断,可省略皮肤试验。如果实验室诊断和皮肤试验均未得出确凿结果,可进行额外的细胞检测。HV过敏的治疗包括预防再次接触、患者在再次蜇刺时的自我治疗措施(包括使用急救药物)以及VIT。对于I级SAR且不存在其他重复蜇刺暴露或更严重过敏反应危险因素的情况,无需开具肾上腺素自动注射器(AAI)或给予VIT。在某些情况下,即使既往有I级过敏反应,也可给予VIT,例如存在其他危险因素或不进行VIT会降低生活质量。医生应了解VIT的禁忌证,尽管在权衡利弊后个别合理情况下可予以 override。使用β受体阻滞剂和ACE抑制剂并非VIT的禁忌证。应告知患者可能的相互作用。对于VIT,应根据患者病史和过敏诊断结果使用引发疾病的毒液提取物。如果存在双重致敏且触发因素病史不明确,即使采用额外的诊断程序也无法确定罪魁祸首毒液,应使用两种毒液提取物进行VIT。VIT的标准维持剂量为100 μg HV。对于有蜜蜂毒液过敏且蜇刺暴露风险增加或过敏反应特别严重的成年患者,可从VIT开始时就考虑给予200 μg的维持剂量。可考虑给予非镇静性H1受体阻断抗组胺药以减少副作用。维持剂量应在第一年每4周给药一次,从第二年起,根据所用制剂,按照制造商说明每5 - 6周给药一次;如果使用长效制剂,从第三年起间隔可延长至8周。如果在VIT期间发生显著的复发性全身反应,临床医生应识别并尽可能消除促进这些反应的协同因素。如果无法做到这一点或不存在此类协同因素,如果预防性给予H1受体阻断抗组胺药无效,且更高剂量的VIT未导致VIT耐受,医生应考虑使用抗IgE抗体(如奥马珠单抗)进行额外治疗,作为非标签使用。出于实际原因,只有少数患者能够接受蜇刺激发试验以检查治疗效果,这需要住院监测和应急待命。要进行此类激发试验,患者必须耐受计划的维持剂量的VIT。在用ACE抑制剂治疗时如果治疗失败,医生应考虑停用ACE抑制剂。在未诱导耐受的情况下,医生应增加维持剂量(成人从200 μg增加至最大400 μg,儿童最大200 μg HV)。如果增加维持剂量不能提供足够的保护且存在严重过敏反应的危险因素,医生应考虑在昆虫活动季节联合使用基于抗IgE抗体(奥马珠单抗;非标签使用)的药物。对于无特定危险因素的患者,如果维持治疗已耐受且无复发性过敏事件,3 - 5年后可停用VIT。对于肥大细胞增多症患者、因膜翅目昆虫蜇刺导致心血管或呼吸骤停病史(严重程度IV级)或与复发性和/或严重SAR个体风险增加相关的其他特定情况(如遗传性α - 类胰蛋白酶血症),可考虑延长或永久进行VIT。在昆虫暴露强烈且不可避免增加的情况下,成人可接受VIT直至密切接触结束。对于有I级和II级SAR病史的患者,当达到并耐受VIT的维持剂量时,如果不存在其他危险因素,可省略AAI的处方。在常规治疗期后VIT终止后同样如此。有≥ III级反应病史的患者,或II级反应合并增加无反应或重复严重蜇刺反应风险的其他因素的患者,在VIT期间及VIT常规终止后应携带急救包,包括AAI。