Shavadia Jay S, Stanberry Larissa, Singh Jyotpal, Thao Kiahltone R, Ghasemzadeh Nima, Mercado Nestor, Nayak Keshav R, Alraies M Chadi, Bagur Rodrigo, Saw Jacqueline, Bagai Akshay, Bainey Kevin R, Madan Mina, Amlani Shy, Garberich Ross, Grines Cindy L, Garcia Santiago, Henry Timothy D, Dehghani Payam
Division of Cardiology, Department of Medicine, University of Saskatchewan, Saskatoon, Saskatchewan, Canada.
Minneapolis Heart Institute Foundation, Minneapolis, Minnesota.
J Soc Cardiovasc Angiogr Interv. 2023 Jun 21;2(5):100970. doi: 10.1016/j.jscai.2023.100970.
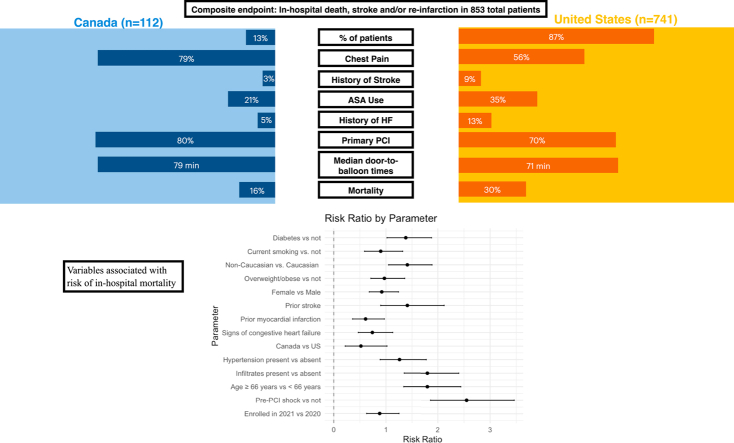
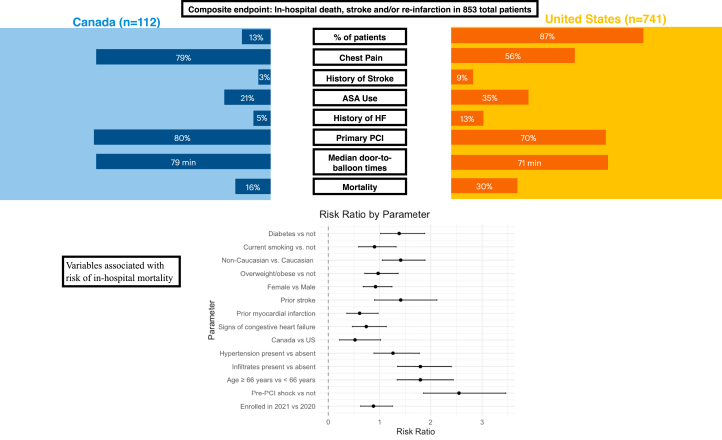
Important health care differences exist between the United States (US) and Canada, which may have been exacerbated during the pandemic. We compared clinical characteristics, treatment strategies, and clinical outcomes of patients with ST-segment elevation myocardial infarction (STEMI) and COVID-19 (STEMI-COVID) treated in the US and Canada.
The North American COVID-19 Myocardial Infarction registry is a prospective, investigator-initiated study enrolling patients with STEMI with confirmed or suspected COVID-19 in the US and Canada. The primary end point was in-hospital mortality. Additionally, we explored associations between vaccination and clinical outcomes.
Of 853 patients with STEMI-COVID, 112 (13%) were enrolled in Canada, and compared with the US, patients in Canada were more likely to present with chest pain and less likely to have a history of heart failure, stroke/transient ischemic attack, pulmonary infiltrates or renal failure. In both countries, the primary percutaneous coronary intervention was the dominant reperfusion strategy, with no difference in door-to-balloon times; fibrinolysis was used less frequently in the US than in Canada. The adjusted in-hospital mortality was not different between the 2 countries (relative risk [RR], 1.0; 95% CI, 0.46-2.72; = 1.0). However, the risk of in-hospital mortality was significantly higher in unvaccinated compared with vaccinated patients with STEMI-COVID (RR, 4.7; 95% CI, 1.7-11.53; = .015).
Notable differences in morbidities and reperfusion strategies were evident between patients with STEMI-COVID in the US compared with Canada. No differences were noted for in-hospital mortality. Vaccination, regardless of region, appeared to associate with a lower risk of in-hospital mortality strongly.
美国和加拿大在医疗保健方面存在重要差异,在疫情期间这些差异可能进一步加剧。我们比较了在美国和加拿大接受治疗的ST段抬高型心肌梗死(STEMI)合并2019冠状病毒病(COVID-19)患者(STEMI-COVID)的临床特征、治疗策略和临床结局。
北美COVID-19心肌梗死登记研究是一项由研究者发起的前瞻性研究,纳入美国和加拿大确诊或疑似COVID-19的STEMI患者。主要终点是住院死亡率。此外,我们探讨了疫苗接种与临床结局之间的关联。
在853例STEMI-COVID患者中,112例(13%)在加拿大登记入组。与美国患者相比,加拿大患者更易出现胸痛,且患心力衰竭、中风/短暂性脑缺血发作、肺部浸润或肾衰竭的病史可能性更小。在两国,主要经皮冠状动脉介入治疗是主要的再灌注策略,门球时间无差异;美国使用纤维蛋白溶解疗法的频率低于加拿大。两国调整后的住院死亡率无差异(相对风险[RR],1.0;95%置信区间[CI],0.46 - 2.72;P = 1.0)。然而,与接种疫苗的STEMI-COVID患者相比,未接种疫苗患者的住院死亡风险显著更高(RR,4.7;95%CI,1.7 - 11.53;P = 0.015)。
与加拿大相比,美国STEMI-COVID患者在发病率和再灌注策略方面存在显著差异。住院死亡率无差异。无论在哪个地区,疫苗接种似乎都与较低的住院死亡风险密切相关。