Department of Epidemiology, School of Public Health, Nanjing Medical University, Nanjing, 211166, China.
Centre for Global Health, Usher Institute, University of Edinburgh, Edinburgh, UK.
BMC Med. 2023 Jun 26;21(1):224. doi: 10.1186/s12916-023-02932-5.
Statistical modelling studies based on excess morbidity and mortality are important for understanding RSV disease burden for age groups that are less frequently tested for RSV. We aimed to understand the full age spectrum of RSV morbidity and mortality burden based on statistical modelling studies, as well as the value of modelling studies in RSV disease burden estimation.
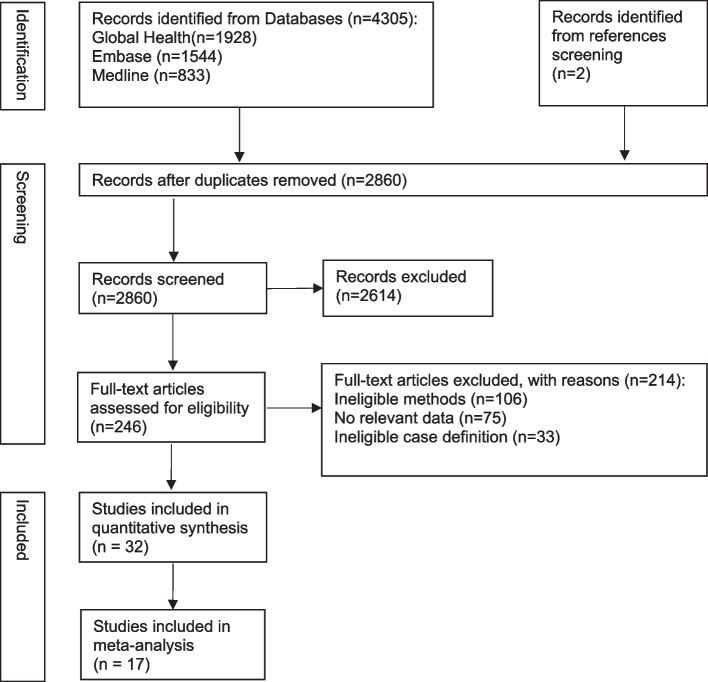
The databases Medline, Embase and Global Health were searched to identify studies published between January 1, 1995, and December 31, 2021, reporting RSV-associated excess hospitalisation or mortality rates of any case definitions using a modelling approach. All reported rates were summarised using median, IQR (Interquartile range) and range by age group, outcome and country income group; where applicable, a random-effects meta-analysis was conducted to combine the reported rates. We further estimated the proportion of RSV hospitalisations that could be captured in clinical databases.
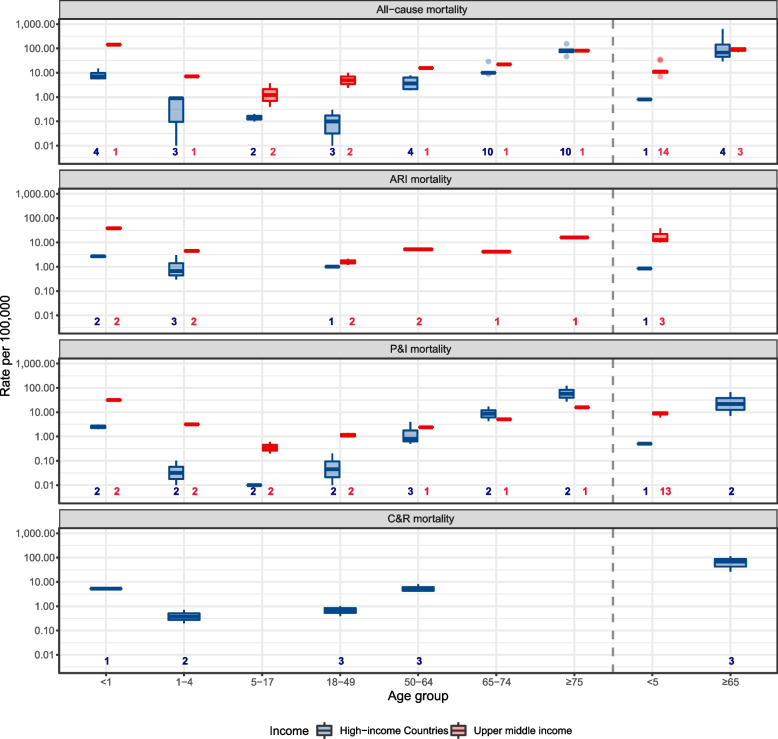
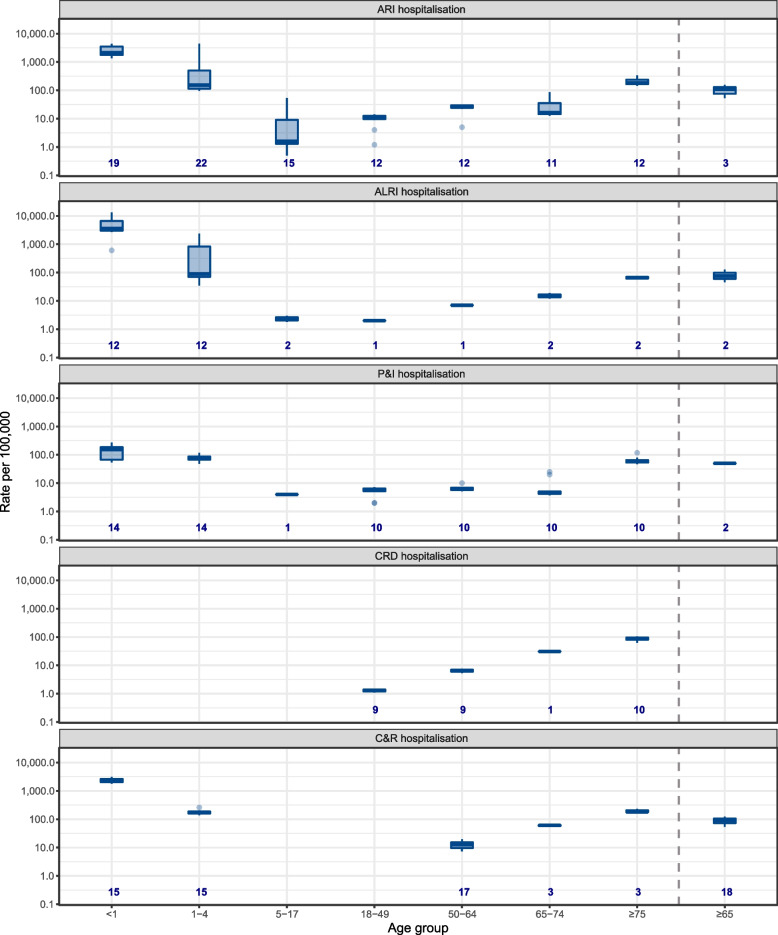
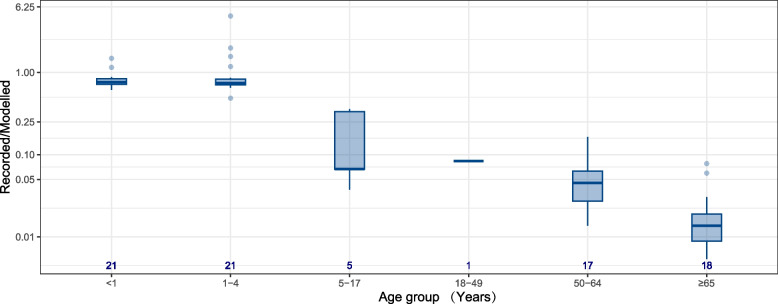
A total of 32 studies were included, with 26 studies from high-income countries. RSV-associated hospitalisation and mortality rates both showed a U-shape age pattern. Lowest and highest RSV acute respiratory infection (ARI) hospitalisation rates were found in 5-17 years (median: 1.6/100,000 population, IQR: 1.3-18.5) and < 1 year (2235.7/100,000 population, 1779.1-3552.5), respectively. Lowest and highest RSV mortality rates were found in 18-49 years (0.1/100,000 population, 0.06-0.2) and ≥ 75 years (80.0/100,000 population, 70.0-90.0) for high-income countries, respectively, and in 18-49 years (0.3/100,000 population, 0.1-2.4) and < 1 year (143.4/100,000 population, 143.4-143.4) for upper-middle income countries. More than 70% of RSV hospitalisations in children < 5 years could be captured in clinical databases whereas less than 10% of RSV hospitalisations could be captured in adults, especially for adults ≥ 50 years. Using pneumonia and influenza (P&I) mortality could potentially capture half of all RSV mortality in older adults but only 10-30% of RSV mortality in children.
Our study provides insights into the age spectrum of RSV hospitalisation and mortality. RSV disease burden using laboratory records alone could be substantially severely underreported for age groups ≥ 5 years. Our findings confirm infants and older adults should be prioritised for RSV immunisation programmes.
PROSPERO CRD42020173430.
基于超额发病率和死亡率的统计建模研究对于了解发病率和死亡率较低的年龄组的 RSV 疾病负担非常重要。我们旨在通过统计建模研究了解 RSV 发病率和死亡率负担的完整年龄范围,以及建模研究在 RSV 疾病负担估计中的价值。
检索 Medline、Embase 和 Global Health 数据库,以确定 1995 年 1 月 1 日至 2021 年 12 月 31 日期间发表的研究,这些研究使用建模方法报告了任何病例定义的 RSV 相关超额住院或死亡率。按年龄组、结局和国家收入组汇总所有报告的比率;在适用的情况下,采用随机效应荟萃分析合并报告的比率。我们还估计了可以在临床数据库中捕获的 RSV 住院治疗的比例。
共纳入 32 项研究,其中 26 项来自高收入国家。与 RSV 相关的住院和死亡率均呈 U 形年龄模式。5-17 岁(中位数:1.6/100,000 人,IQR:1.3-18.5)和<1 岁(2235.7/100,000 人,1779.1-3552.5)的 RSV 急性呼吸道感染(ARI)住院率最低和最高。高收入国家 RSV 死亡率最低和最高的年龄组分别为 18-49 岁(0.1/100,000 人,0.06-0.2)和≥75 岁(80.0/100,000 人,70.0-90.0),中上收入国家分别为 18-49 岁(0.3/100,000 人,0.1-2.4)和<1 岁(143.4/100,000 人,143.4-143.4)。儿童<5 岁的 RSV 住院治疗中,超过 70%可以在临床数据库中捕获,而成年人,尤其是 50 岁以上的成年人,只有不到 10%的 RSV 住院治疗可以捕获。使用肺炎和流感(P&I)死亡率可以潜在地捕获老年人中一半的所有 RSV 死亡率,但只能捕获儿童中 10-30%的 RSV 死亡率。
我们的研究提供了 RSV 住院和死亡的年龄谱的见解。仅使用实验室记录报告的 RSV 疾病负担对于≥5 岁的年龄组可能严重低估。我们的研究结果证实,婴儿和老年人应优先考虑 RSV 免疫接种计划。
PROSPERO CRD42020173430。