Mekontso Dessap Armand, Papazian Laurent, Schaller Manuella, Nseir Saad, Megarbane Bruno, Haudebourg Luc, Timsit Jean-François, Teboul Jean-Louis, Kuteifan Khaldoun, Gainnier Marc, Slama Michel, Houeto Patrick, Lecourt Laurent, Mercat Alain, Vieillard-Baron Antoine
Service de Médecine Intensive Réanimation, Hôpitaux Universitaires Henri-Mondor, AP-HP, 94010, Créteil, France.
CARMAS research group, Univ Paris Est Créteil, Faculté de Santé, 94010, Créteil, France.
Ann Intensive Care. 2023 Jun 27;13(1):57. doi: 10.1186/s13613-023-01150-9.
Inhaled nitric oxide (iNO) has been widely used in patients with COVID-19-related acute respiratory distress syndrome (C-ARDS), though its physiological effects and outcome are debated in this setting. The objective of this cohort study was to describe the modalities of iNO use, clinical response, and outcomes in a large cohort of C-ARDS patients.
Multicentre, retrospective cohort study conducted in France.
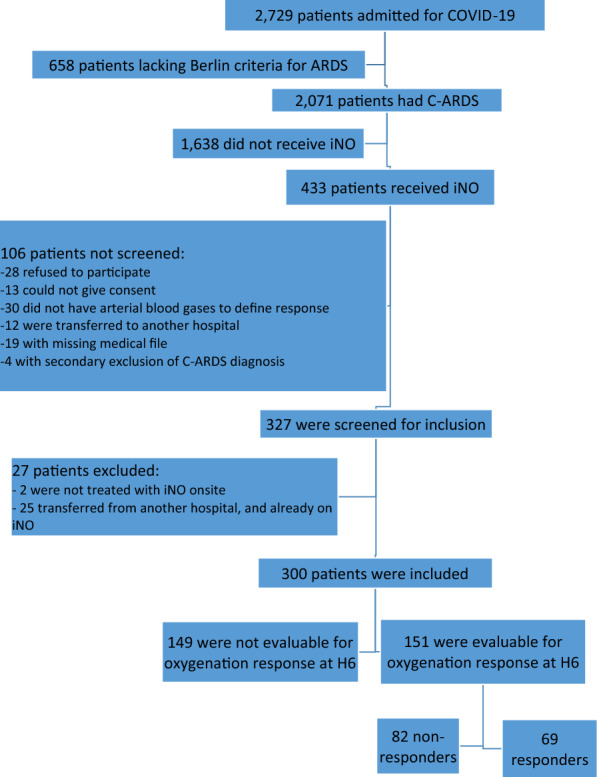
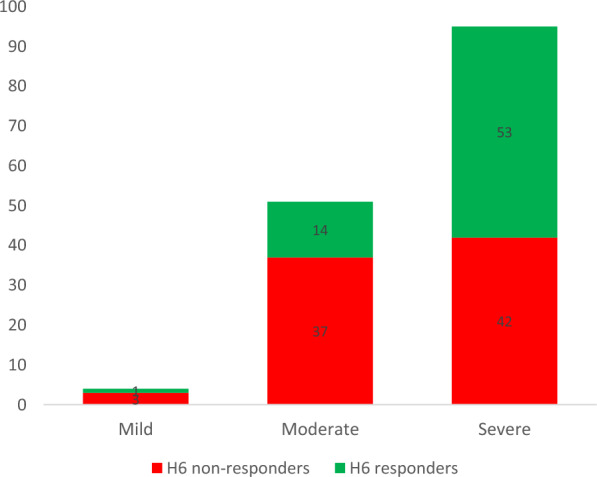
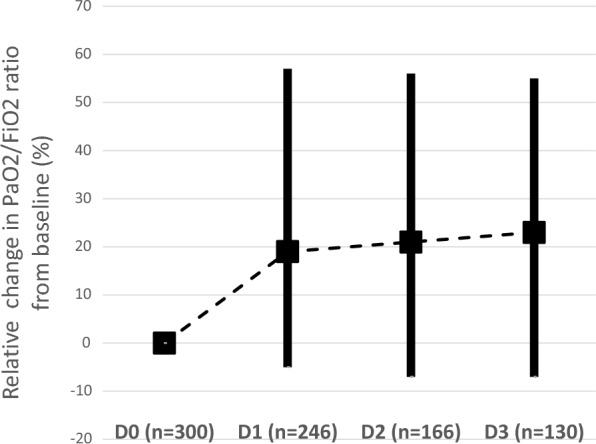
From end February to December 2020, 300 patients (22.3% female) were included, 84.5% were overweight and 69.0% had at least one comorbidity. At ICU admission, their median (IQR) age, SAPS II, and SOFA score were 66 (57-72) years, 37 (29-48), and 5 (3-8), respectively. Patients were all ventilated according to a protective ventilation strategy, and 68% were prone positioned before iNO initiation. At iNO initiation, 2%, 37%, and 61% of patients had mild, moderate, and severe ARDS, respectively. The median duration of iNO treatment was 2.8 (1.1-5.5) days with a median dosage of 10 (7-13) ppm at initiation. Responders (PaO/FiO ratio improving by 20% or more) represented 45.7% of patients at 6 h from iNO initiation. The severity of ARDS was the only predictive factor associated with iNO response. Among all evaluable patients, the crude mortality was not significantly different between responders at 6 h and their counterparts. Of the 62 patients with refractory ARDS (who fulfilled extracorporeal membrane oxygenation criteria before iNO initiation), 32 (51.6%) no longer fulfilled these criteria after 6 h of iNO. The latter showed significantly lower mortality than the other half (who remained ECMO eligible), including after confounder adjustment (adjusted OR: 0.23, 95% CI 0.06, 0.89, p = 0.03).
Our study reports the benefits of iNO in improving arterial oxygenation in C-ARDS patients. This improvement seems more relevant in the most severe cases. In patients with ECMO criteria, an iNO-driven improvement in gas exchange was associated with better survival. These results must be confirmed in well-designed prospective studies.
吸入一氧化氮(iNO)已广泛应用于新型冠状病毒肺炎相关急性呼吸窘迫综合征(C-ARDS)患者,但其在此情况下的生理效应和预后仍存在争议。本队列研究的目的是描述一大群C-ARDS患者使用iNO的方式、临床反应和预后。
在法国进行的多中心回顾性队列研究。
从2020年2月底至12月,纳入300例患者(22.3%为女性),84.5%超重,69.0%至少有一种合并症。入住重症监护病房(ICU)时,他们的年龄中位数(四分位间距)、简化急性生理学评分(SAPS)II和序贯器官衰竭评估(SOFA)评分分别为66(57 - 72)岁、37(29 - 48)和5(3 - 8)。所有患者均按照保护性通气策略进行通气,68%在开始使用iNO前采用俯卧位。开始使用iNO时,2%、37%和61%的患者分别患有轻度、中度和重度ARDS。iNO治疗的中位持续时间为2.8(1.1 - 5.5)天,开始时的中位剂量为10(7 - 13)ppm。在开始使用iNO后6小时,反应者(动脉血氧分压/吸入氧分数值改善20%或更多)占患者的45.7%。ARDS的严重程度是与iNO反应相关的唯一预测因素。在所有可评估的患者中,6小时时反应者与非反应者的粗死亡率无显著差异。在62例难治性ARDS患者(在开始使用iNO前符合体外膜肺氧合标准)中,32例(51.6%)在使用iNO 6小时后不再符合这些标准。后者的死亡率显著低于另一半(仍符合体外膜肺氧合标准者),包括在进行混杂因素调整后(调整后的比值比:0.23,95%置信区间0.06,0.89,p = 0.03)。
我们的研究报告了iNO在改善C-ARDS患者动脉氧合方面的益处。这种改善在最严重的病例中似乎更显著。在符合体外膜肺氧合标准的患者中,iNO驱动的气体交换改善与更好的生存率相关。这些结果必须在设计良好的前瞻性研究中得到证实。