Pharmaceutical Care Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia.
College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia.
Crit Care. 2022 Oct 3;26(1):304. doi: 10.1186/s13054-022-04158-y.
Inhaled nitric oxide (iNO) is used as rescue therapy in patients with refractory hypoxemia due to severe COVID-19 acute respiratory distress syndrome (ARDS) despite the recommendation against the use of this treatment. To date, the effect of iNO on the clinical outcomes of critically ill COVID-19 patients with moderate-to-severe ARDS remains arguable. Therefore, this study aimed to evaluate the use of iNO in critically ill COVID-19 patients with moderate-to-severe ARDS.
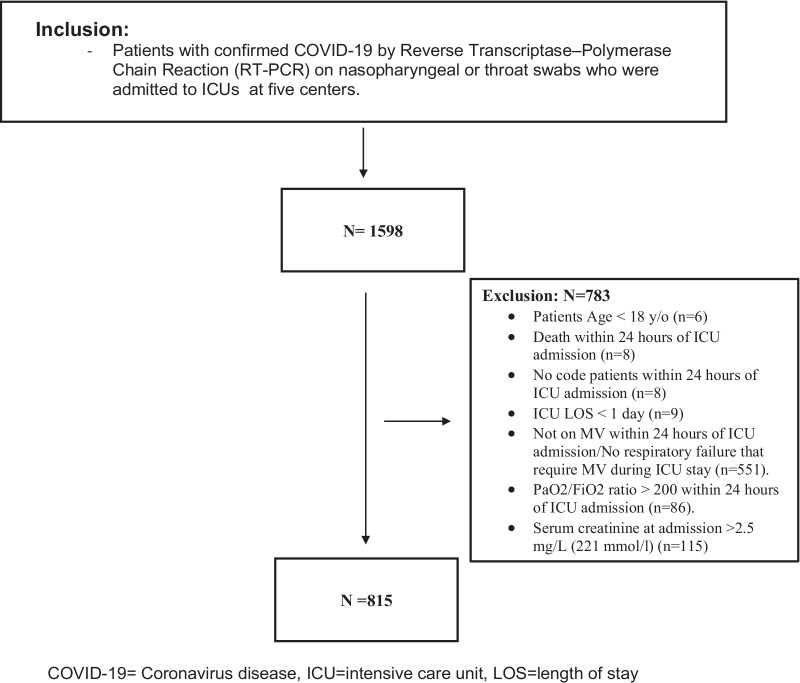
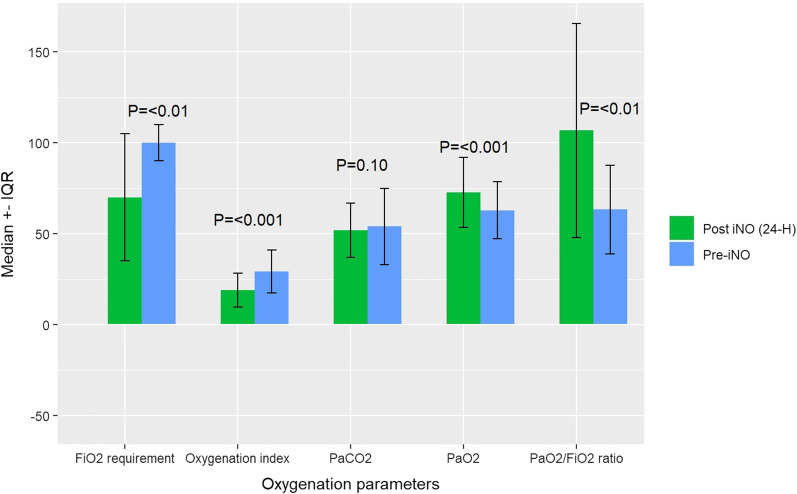
This multicenter, retrospective cohort study included critically ill adult patients with confirmed COVID-19 treated from March 01, 2020, until July 31, 2021. Eligible patients with moderate-to-severe ARDS were subsequently categorized into two groups based on inhaled nitric oxide (iNO) use throughout their ICU stay. The primary endpoint was the improvement in oxygenation parameters 24 h after iNO use. Other outcomes were considered secondary. Propensity score matching (1:2) was used based on the predefined criteria.
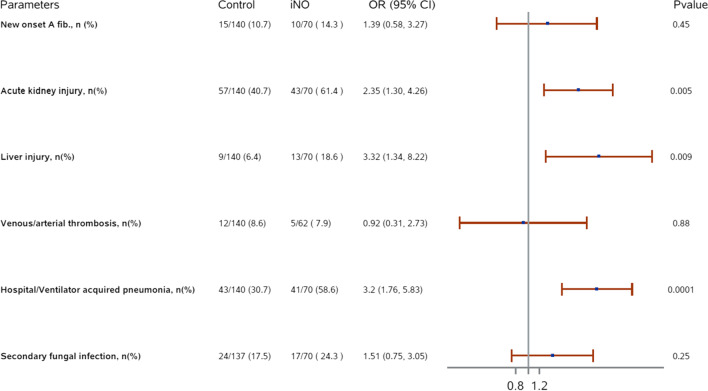
A total of 1598 patients were screened, and 815 were included based on the eligibility criteria. Among them, 210 patients were matched based on predefined criteria. Oxygenation parameters (PaO, FiO requirement, P/F ratio, oxygenation index) were significantly improved 24 h after iNO administration within a median of six days of ICU admission. However, the risk of 30-day and in-hospital mortality were found to be similar between the two groups (HR: 1.18; 95% CI: 0.77, 1.82; p = 0.45 and HR: 1.40; 95% CI: 0.94, 2.11; p= 0.10, respectively). On the other hand, ventilator-free days (VFDs) were significantly fewer, and ICU and hospital LOS were significantly longer in the iNO group. In addition, patients who received iNO had higher odds of acute kidney injury (AKI) (OR (95% CI): 2.35 (1.30, 4.26), p value = 0.005) and hospital/ventilator-acquired pneumonia (OR (95% CI): 3.2 (1.76, 5.83), p value = 0.001).
In critically ill COVID-19 patients with moderate-to-severe ARDS, iNO rescue therapy is associated with improved oxygenation parameters but no mortality benefits. Moreover, iNO use is associated with higher odds of AKI, pneumonia, longer LOS, and fewer VFDs.
尽管不建议使用吸入一氧化氮(iNO)治疗,但在重度 COVID-19 急性呼吸窘迫综合征(ARDS)导致的难治性低氧血症患者中,iNO 仍被用作抢救治疗。迄今为止,iNO 对患有中度至重度 ARDS 的危重症 COVID-19 患者的临床结局的影响仍存在争议。因此,本研究旨在评估 iNO 在患有中度至重度 ARDS 的危重症 COVID-19 患者中的应用。
这是一项多中心、回顾性队列研究,纳入了 2020 年 3 月 1 日至 2021 年 7 月 31 日期间接受治疗的确诊 COVID-19 的成年危重症患者。随后,根据吸入一氧化氮(iNO)在整个 ICU 期间的使用情况,将符合条件的中度至重度 ARDS 患者分为两组。主要终点是 iNO 使用后 24 小时氧合参数的改善。其他结果被认为是次要的。根据预设标准,使用倾向评分匹配(1:2)。
共筛选了 1598 名患者,根据入选标准,815 名患者入选。其中,根据预设标准,210 名患者进行了匹配。在 ICU 入院中位 6 天内接受 iNO 治疗后 24 小时,氧合参数(PaO、FiO 需求、P/F 比、氧合指数)显著改善。然而,两组 30 天和住院死亡率的风险相似(HR:1.18;95%CI:0.77,1.82;p=0.45 和 HR:1.40;95%CI:0.94,2.11;p=0.10)。另一方面,iNO 组的无呼吸机天数(VFDs)明显减少,ICU 和住院时间明显延长。此外,接受 iNO 治疗的患者发生急性肾损伤(AKI)的几率更高(OR(95%CI):2.35(1.30,4.26),p 值=0.005)和医院/呼吸机相关性肺炎(OR(95%CI):3.2(1.76,5.83),p 值=0.001)。
在患有中度至重度 ARDS 的危重症 COVID-19 患者中,iNO 抢救治疗可改善氧合参数,但不能改善死亡率。此外,iNO 的使用与 AKI、肺炎、更长的 LOS 和更少的 VFDs 的发生几率更高有关。