Harborg Sixten, Feldt Maria, Cronin-Fenton Deirdre, Klintman Marie, Dalton Susanne O, Rosendahl Ann H, Borgquist Signe
Department of Oncology, Aarhus University/Aarhus University Hospital, Entrance C, Level 1, C106, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
Department of Clinical Epidemiology, Aarhus University, Aarhus, Denmark.
Cancer Metab. 2023 Jun 27;11(1):8. doi: 10.1186/s40170-023-00308-0.
Examine the association between obesity and clinical outcomes in early breast cancer and assess if patient, tumor, and treatment characteristics modify such associations in Malmö Diet and Cancer Study patients (MDCS).
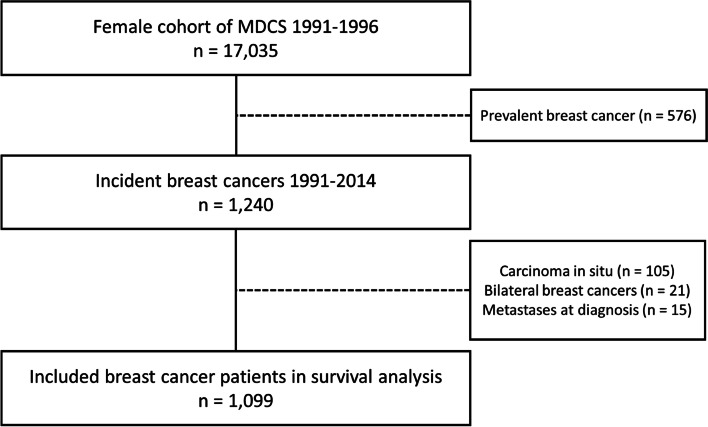
The MDCS enrolled 17,035 Swedish women from 1991 to 1996. At enrollment, participants' body mass index (BMI), waist circumference and body fat percentage measures were collected. We identified all female MDCS participants with invasive breast cancer from 1991 to 2014. Follow-up began at breast cancer diagnosis and ended at breast cancer recurrence (BCR), death, emigration, or June 8, 2020. The World Health Organization guidelines were used to classify BMI, waist circumference, and body fat percentage into three categories of healthy weight, overweight, and obesity. We fit Cox regression models to compute adjusted hazard ratios (HRs) with 95% confidence intervals (CI) of BCR according to body composition. To evaluate effect measure modification, we stratified Cox models by patient, tumor, and treatment characteristics.
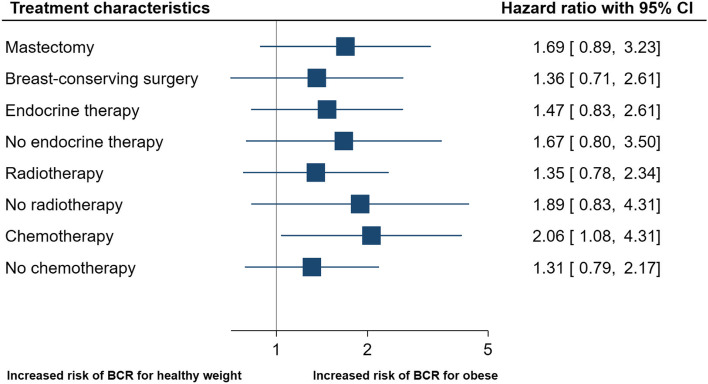
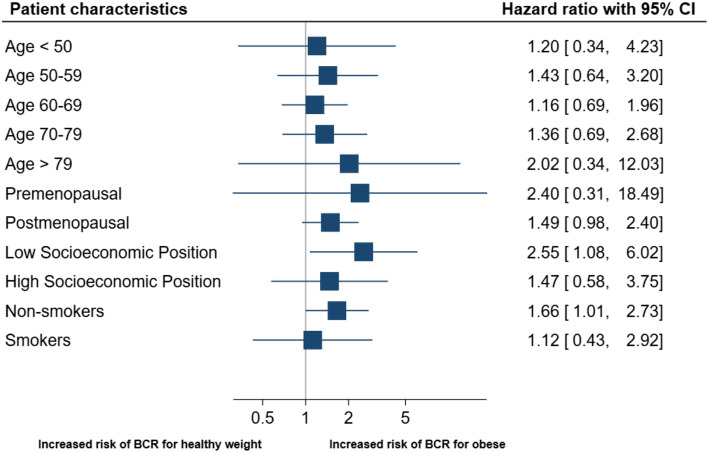
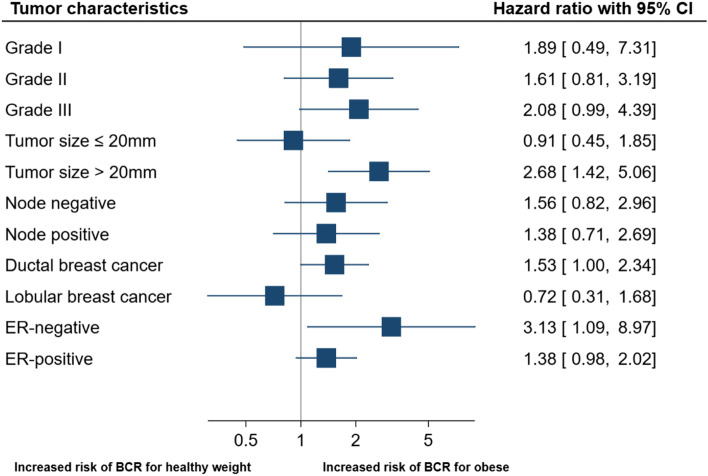
In total, 263 BCRs were diagnosed over 12,816 person-years among 1099 breast cancer patients with a median follow-up of 11.1 years. Obesity according to BMI (HR = 1.44 [95%CI 1.00-2.07]), waist circumference (HR = 1.31 [95%CI 0.98-1.77]), and body fat percentage (HR = 1.41 [95%CI 1.02-1.98]) was associated with increased risk of BCR compared with healthy weight. Obesity was stronger associated with BCR in patients with low socioeconomic position (HR = 2.55 [95%CI 1.08-6.02]), larger tumors > 20 mm (HR = 2.68 [95%CI 1.42-5.06]), estrogen-receptor-negative breast cancer (HR = 3.13 [95%CI 1.09-8.97]), and with adjuvant chemotherapy treatment (HR = 2.06 [95%CI 1.08-4.31]).
Higher pre-diagnostic BMI, waist circumference, and body fat percentage was associated with increased risk of BCR. The association between obesity and BCR appears dependent on patient, tumor, and treatment characteristics.
研究早期乳腺癌患者肥胖与临床结局之间的关联,并评估在马尔默饮食与癌症研究(MDCS)患者中,患者、肿瘤及治疗特征是否会改变这种关联。
MDCS在1991年至1996年期间招募了17035名瑞典女性。在入组时,收集了参与者的体重指数(BMI)、腰围和体脂百分比数据。我们确定了1991年至2014年期间所有患有浸润性乳腺癌的女性MDCS参与者。随访从乳腺癌诊断开始,至乳腺癌复发(BCR)、死亡、移民或2020年6月8日结束。采用世界卫生组织的指南将BMI、腰围和体脂百分比分为健康体重、超重和肥胖三类。我们拟合Cox回归模型,根据身体组成计算BCR的调整风险比(HR)及95%置信区间(CI)。为评估效应测量修正,我们根据患者、肿瘤和治疗特征对Cox模型进行分层。
在1099例乳腺癌患者中,随访12816人年,共诊断出263例BCR,中位随访时间为11.1年。与健康体重相比,根据BMI(HR = 1.44 [95%CI 1.00 - 2.07])、腰围(HR = 1.31 [95%CI 0.98 - 1.77])和体脂百分比(HR = 1.41 [95%CI 1.02 - 1.98])定义的肥胖与BCR风险增加相关。在社会经济地位较低的患者(HR = 2.55 [95%CI 1.08 - 6.02])、肿瘤较大(> 20 mm)(HR = 2.68 [95%CI 1.42 - 5.06])、雌激素受体阴性乳腺癌(HR = 3.13 [95%CI 1.09 - 8.97])以及接受辅助化疗的患者(HR = 2.06 [95%CI 1.08 - 4.31])中,肥胖与BCR的关联更强。
诊断前较高的BMI、腰围和体脂百分比与BCR风险增加相关。肥胖与BCR之间的关联似乎取决于患者、肿瘤和治疗特征。