Di Lullo Luca, Lavalle Carlo, Scatena Alessia, Mariani Marco Valerio, Ronco Claudio, Bellasi Antonio
Department of Nephrology and Dialysis, L. Parodi-Delfino Hospital, 00034 Colleferro, Italy.
Department of Clinical, Internal, Anesthesiologist and Cardiovascular Sciences, Sapienza University of Rome, Viale del Policlinico 155, 00161 Rome, Italy.
J Clin Med. 2023 Jun 12;12(12):3992. doi: 10.3390/jcm12123992.
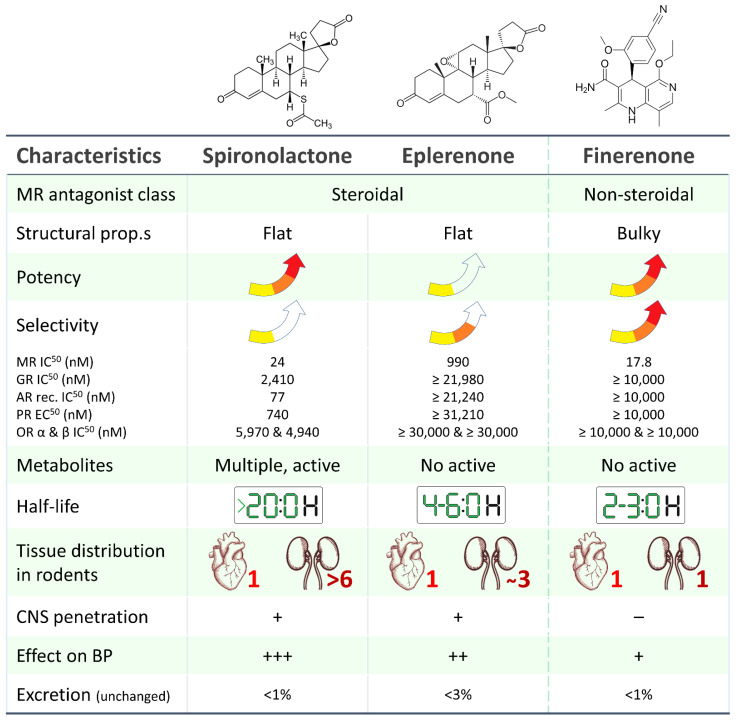
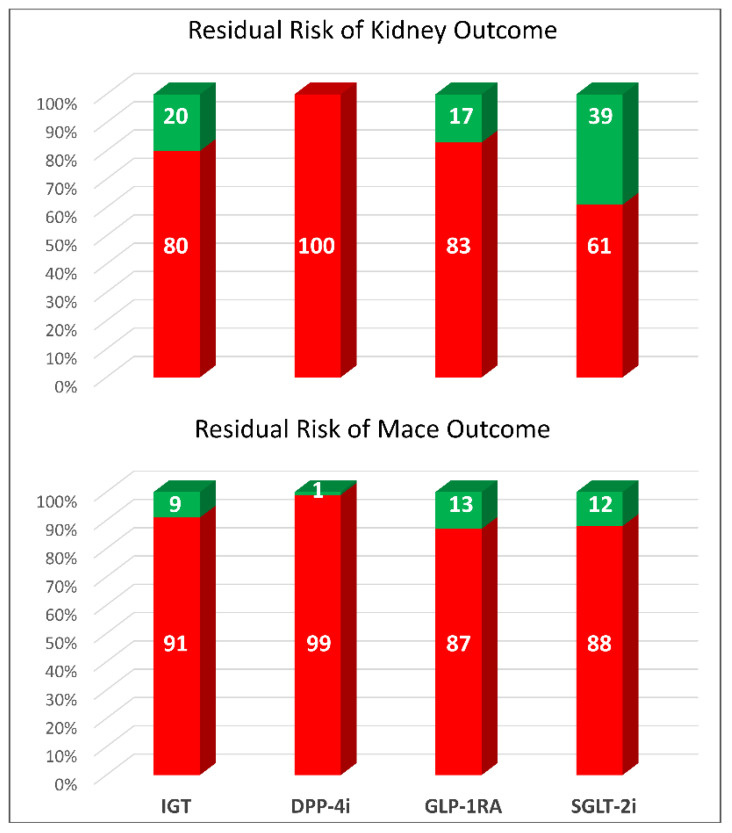
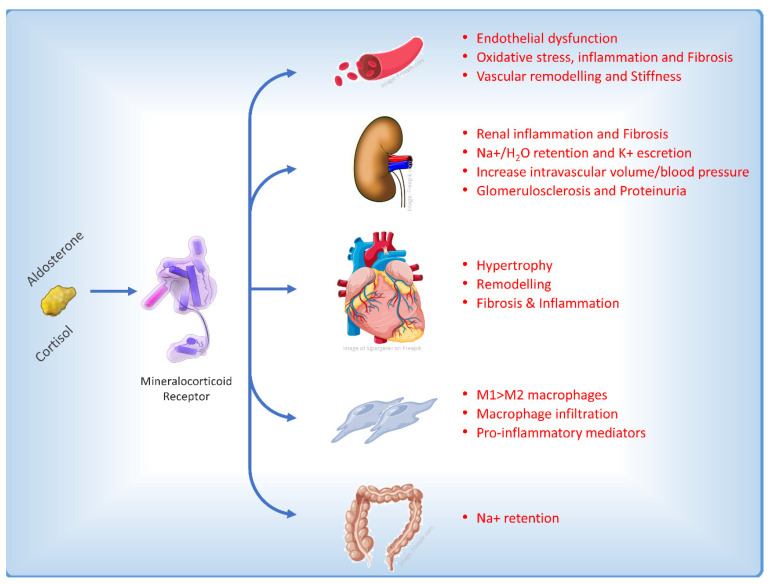
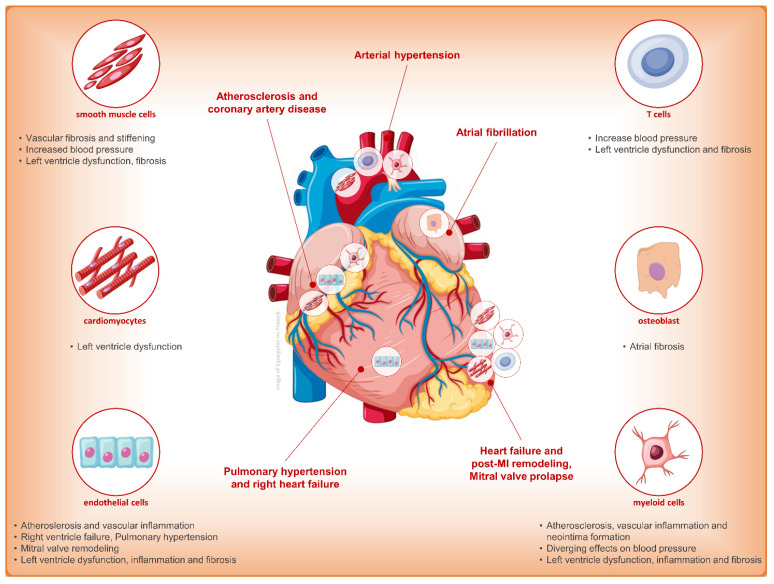
Chronic kidney disease (CKD) is one of the most common complications of diabetes mellitus and an independent risk factor for cardiovascular disease. Despite guideline-directed therapy of CKD in patients with type 2 diabetes, the risk of renal failure and cardiovascular events still remains high, and diabetes remains the leading cause of end-stage kidney disease in affected patients. To date, current medications for CKD and type 2 diabetes mellitus have not reset residual risk in patients due to a high grade of inflammation and fibrosis contributing to kidney and heart disease. This question-and-answer-based review will discuss the pharmacological and clinical differences between finerenone and other mineralocorticoid receptor antagonists and then move on to the main evidence in the cardiovascular and renal fields, closing, finally, on the potential role of therapeutic combination with sodium-glucose cotransporter 2 inhibitors (SGLT2is).
慢性肾脏病(CKD)是糖尿病最常见的并发症之一,也是心血管疾病的独立危险因素。尽管针对2型糖尿病患者的CKD有指南指导的治疗,但肾衰竭和心血管事件的风险仍然很高,糖尿病仍是受影响患者终末期肾病的主要原因。迄今为止,由于导致肾脏和心脏疾病的高度炎症和纤维化,目前用于CKD和2型糖尿病的药物尚未消除患者的残余风险。这篇基于问答的综述将讨论非奈利酮与其他盐皮质激素受体拮抗剂在药理学和临床方面的差异,然后转向心血管和肾脏领域的主要证据,最后阐述与钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)联合治疗的潜在作用。