Department of Pharmacology, College of Medicine, Shaqra University, Shaqra 11961, Saudi Arabia.
Department of Pharmacology, Institute of Basic Medical Sciences, Khyber Medical University, Peshawar 25100, Khyber Pakhtunkhwa, Pakistan.
Medicina (Kaunas). 2023 May 25;59(6):1023. doi: 10.3390/medicina59061023.
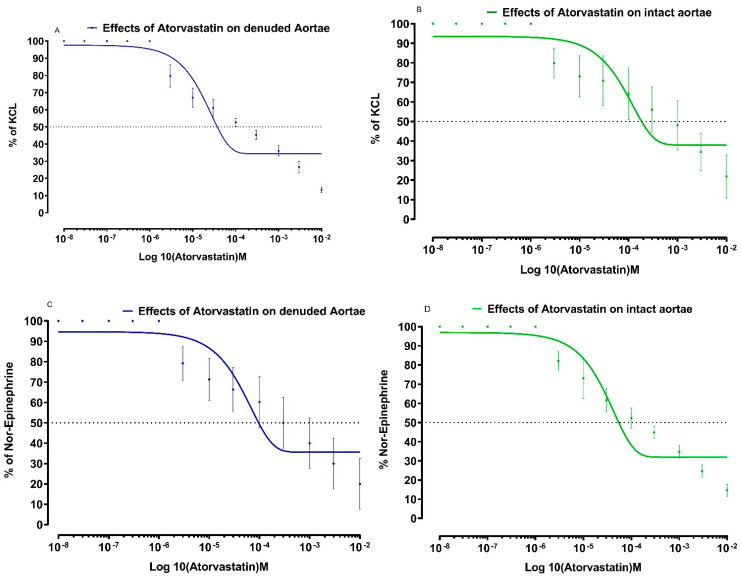
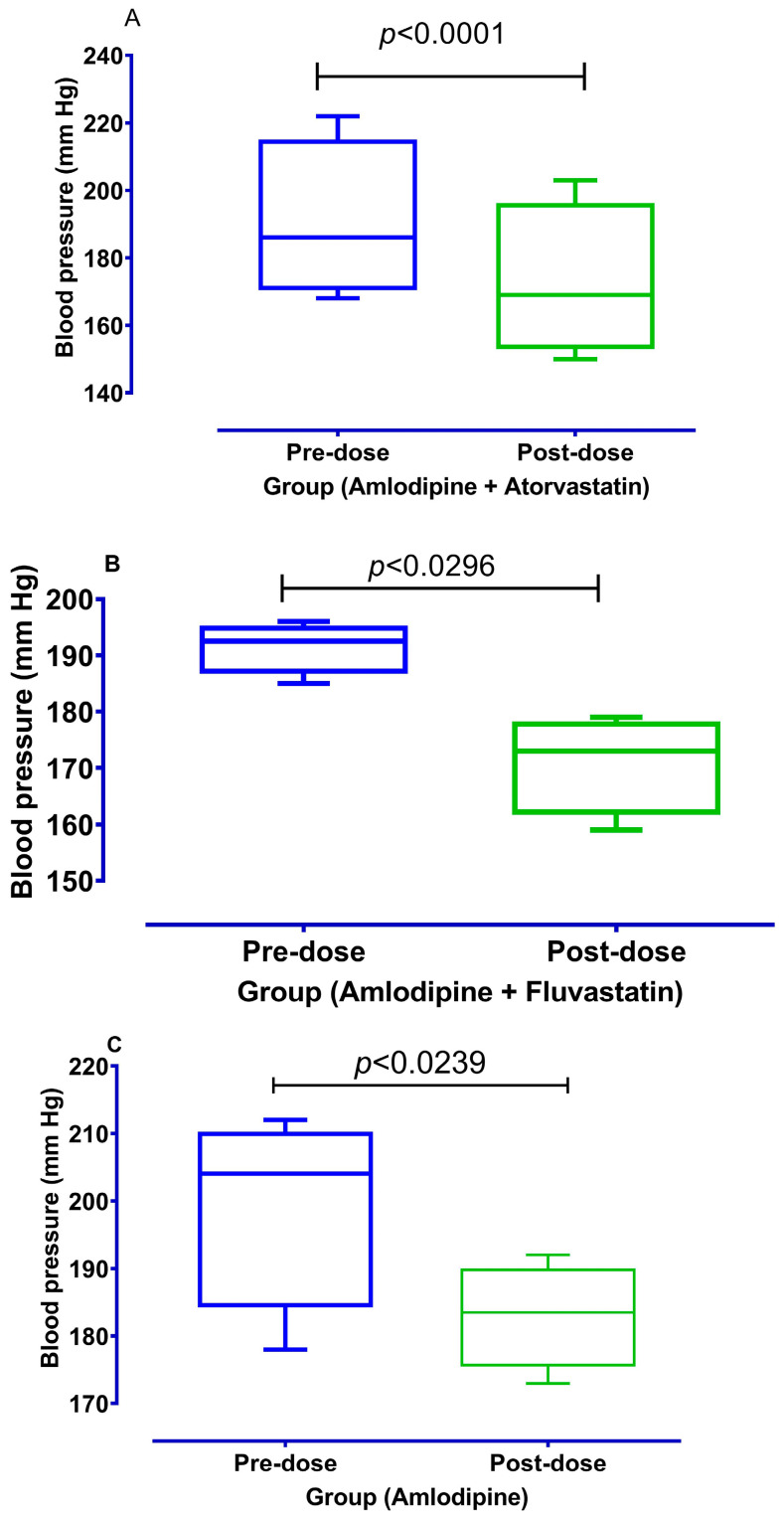
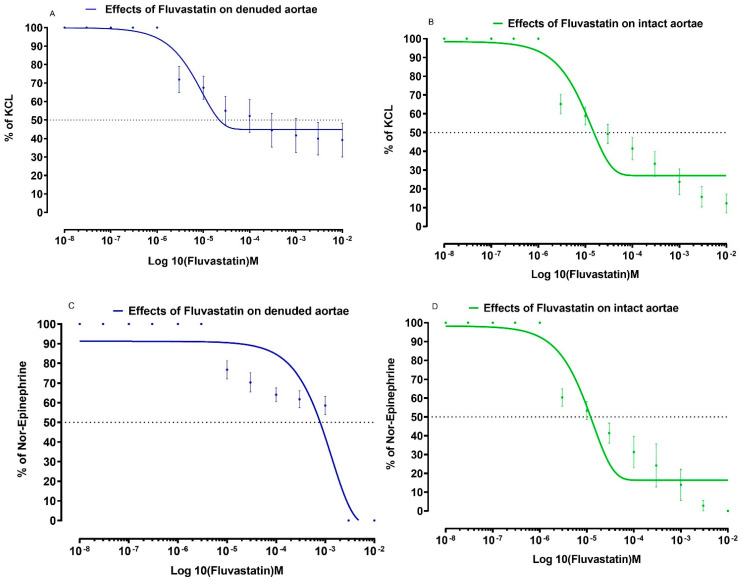
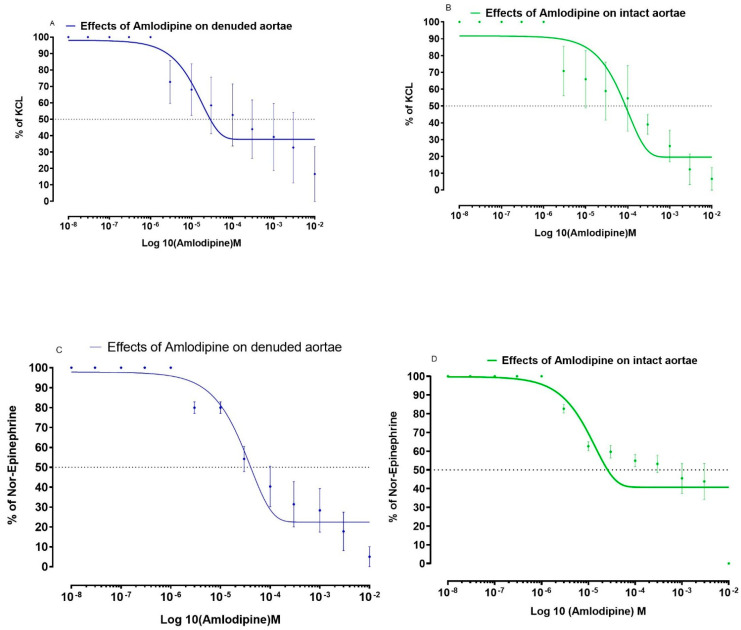
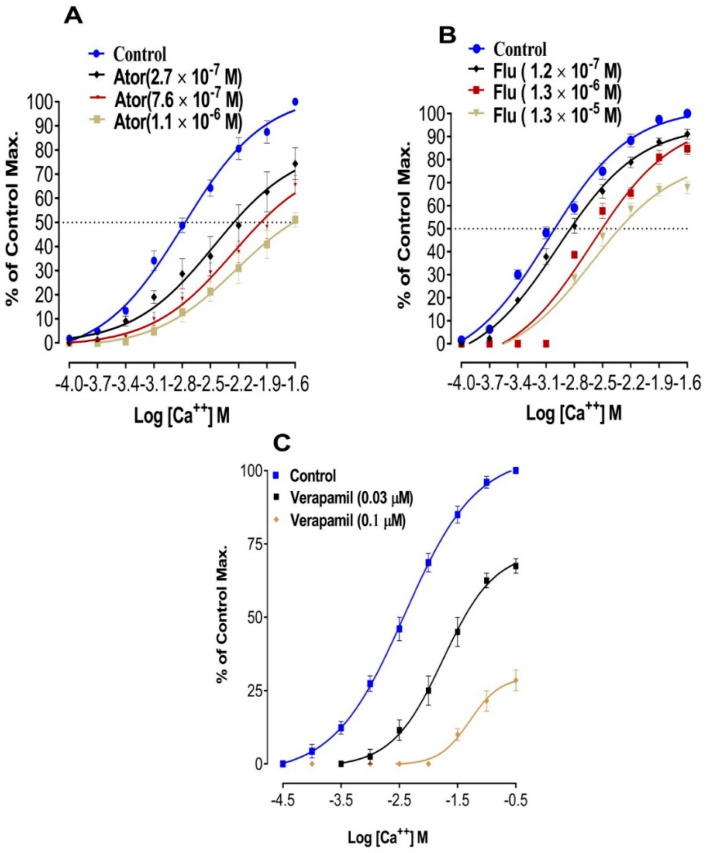
We have recently reported that stains have calcium channel blocking activity in isolated jejunal preparations. In this study, we examined the effects of atorvastatin and fluvastatin on blood vessels for a possible vasorelaxant effect. We also studied the possible additional vasorelaxant effect of atorvastatin and fluvastatin, in the presence of amlodipine, to quantify its effects on the systolic blood pressure of experimental animals. Atorvastatin and fluvastatin were tested in isolated rabbits' aortic strip preparations using 80mM Potassium Chloride (KCl) induced contractions and 1 micro molar Norepinephrine (NE) induced contractions. A positive relaxing effect on 80 mM KCl induced contractions were further confirmed in the absence and presence of atorvastatin and fluvastatin by constructing calcium concentration response curves (CCRCs) while using verapamil as a standard calcium channel blocker. In another series of experiments, hypertension was induced in Wistar rats and different test concentrations of atorvastatin and fluvastatin were administered in their respective EC values to the test animals. A fall in their systolic blood pressure was noted using amlodipine as a standard vasorelaxant drug. The results show that fluvastatin is more potent than amlodipine as it relaxed NE induced contractions where the amplitude reached 10% of its control in denuded aortae. Atorvastatin relaxed KCL induced contractions with an amplitude reaching 34.4% of control response as compared to the amlodipine response, i.e., 39.1%. A right shift in the EC (Log Ca++ M) of Calcium Concentration Response Curves (CCRCs) implies that statins have calcium channel blocking activity. A right shift in the EC of fluvastatin with relatively less EC value (-2.8 Log Ca++ M) in the presence of test concentration (1.2 × 10 M) of fluvastatin implies that fluvastatin is more potent than atorvastatin. The shift in EC resembles the shift of Verapamil, a standard calcium channel blocker (-1.41 Log Ca++ M). Atorvastatin and fluvastatin relax the aortic strip preparations predominantly through the inhibition of voltage gated calcium channels in high molar KCL induced contractions. These statins also inhibit the effects of NE induced contractions. The study also confirms that atorvastatin and fluvastatin potentiate blood pressure lowering effects in hypertensive rats.
我们最近报道称,在分离的空肠制剂中,斑点具有钙通道阻滞活性。在这项研究中,我们研究了阿托伐他汀和氟伐他汀对血管的影响,以观察其可能的血管舒张作用。我们还研究了阿托伐他汀和氟伐他汀在氨氯地平存在下的可能额外血管舒张作用,以量化其对实验动物收缩压的影响。阿托伐他汀和氟伐他汀在分离的兔主动脉带制剂中进行了测试,使用 80mM 氯化钾(KCl)诱导的收缩和 1 微摩尔去甲肾上腺素(NE)诱导的收缩。在没有和存在阿托伐他汀和氟伐他汀的情况下,通过构建钙浓度反应曲线(CCRC)进一步证实了对 80mM KCl 诱导收缩的阳性舒张作用,同时使用维拉帕米作为标准钙通道阻滞剂。在另一系列实验中,在 Wistar 大鼠中诱导高血压,并在各自的 EC 值下将不同浓度的阿托伐他汀和氟伐他汀施用于测试动物。使用氨氯地平作为标准血管舒张药物,观察到收缩压下降。结果表明,氟伐他汀比氨氯地平更有效,因为它放松了去甲肾上腺素诱导的收缩,其幅度达到去内皮主动脉对照的 10%。阿托伐他汀舒张 KCL 诱导的收缩,其幅度达到对照反应的 34.4%,而与氨氯地平反应相比,即 39.1%。钙浓度反应曲线(CCRC)的 EC(Log Ca++ M)右移表明他汀类药物具有钙通道阻滞活性。在测试浓度(1.2×10M)氟伐他汀存在下,氟伐他汀的 EC 右移(-2.8 Log Ca++ M),相对较小的 EC 值表明氟伐他汀比阿托伐他汀更有效。EC 的移位类似于标准钙通道阻滞剂维拉帕米(-1.41 Log Ca++ M)的移位。阿托伐他汀和氟伐他汀主要通过抑制高摩尔 KCL 诱导的收缩中的电压门控钙通道来舒张主动脉带制剂。这些他汀类药物还抑制了去甲肾上腺素诱导的收缩的作用。该研究还证实,阿托伐他汀和氟伐他汀增强了高血压大鼠的降压作用。