MRC Centre for Global Infectious Disease Analysis, Department of Infectious Disease Epidemiology, School of Public Health, Imperial College London, St Mary's Hospital, 2 Norfolk Place, London, W2 1PG, UK.
HIV Prevention Trials Network Modelling Centre, Imperial College London, London, UK.
AIDS Behav. 2023 Dec;27(12):4010-4021. doi: 10.1007/s10461-023-04115-y. Epub 2023 Jul 1.
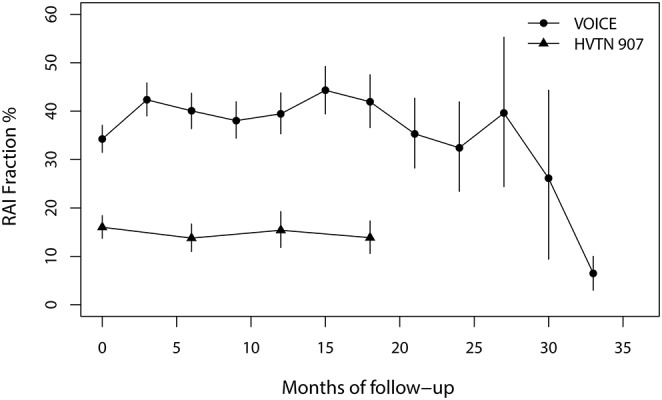
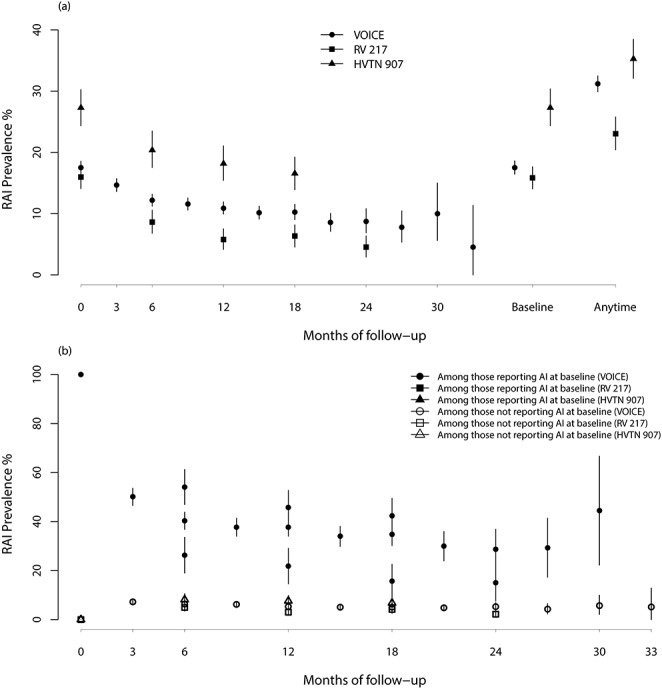
The extent to which receptive anal intercourse (RAI) increases the HIV acquisition risk of women compared to receptive vaginal intercourse (RVI) is poorly understood. We evaluated RAI practice over time and its association with HIV incidence during three prospective HIV cohorts of women: RV217, MTN-003 (VOICE), and HVTN 907. At baseline, 16% (RV 217), 18% (VOICE) of women reported RAI in the past 3 months and 27% (HVTN 907) in the past 6 months, with RAI declining during follow-up by around 3-fold. HIV incidence in the three cohorts was positively associated with reporting RAI at baseline, albeit not always significantly. The adjusted hazard rate ratios for potential confounders (aHR) were 1.1 (95% Confidence interval: 0.8-1.5) for VOICE and 3.3 (1.6-6.8) for RV 217, whereas the ratio of cumulative HIV incidence by RAI practice was 1.9 (0.6-6.0) for HVTN 907. For VOICE, the estimated magnitude of association increased slightly when using a time-varying RAI exposure definition (aHR = 1.2; 0.9-1.6), and for women reporting RAI at every follow-up survey (aHR = 2.0 (1.3-3.1)), though not for women reporting higher RAI frequency (> 30% acts being RAI vs. no RAI in the past 3 months; aHR = 0.7 (0.4-1.1)). Findings indicated precise estimation of the RAI/HIV association, following multiple RVI/RAI exposures, is sensitive to RAI exposure definition, which remain imperfectly measured. Information on RAI practices, RAI/RVI frequency, and condom use should be more systematically and precisely recorded and reported in studies looking at sexual behaviors and HIV seroconversions; standardized measures would aid comparability across geographies and over time.
接受肛交(RAI)相对于阴道交(RVI)会增加女性感染艾滋病毒的风险,但这种风险的程度还不太清楚。我们评估了三个前瞻性艾滋病毒女性队列(RV217、MTN-003[VOICE]和 HVTN 907)中,RAI 随着时间的推移的变化以及与 HIV 发病率之间的关系。在基线时,16%(RV217)、18%(VOICE)的女性报告在过去 3 个月内有过 RAI,27%(HVTN 907)的女性报告在过去 6 个月内有过 RAI,随访期间 RAI 下降了约 3 倍。三个队列的 HIV 发病率与基线时报告 RAI 呈正相关,尽管并不总是具有显著意义。调整潜在混杂因素的调整后危险率比(aHR)为 VOICE 的 1.1(95%置信区间:0.8-1.5)和 RV217 的 3.3(1.6-6.8),而根据 RAI 实践计算的 HIV 累积发病率比为 HVTN 907 的 1.9(0.6-6.0)。对于 VOICE,当使用时变 RAI 暴露定义时,关联的估计幅度略有增加(aHR=1.2;0.9-1.6),对于每次随访调查都报告 RAI 的女性(aHR=2.0(1.3-3.1)),尽管对于报告更高 RAI 频率(>30%的行为是 RAI 与过去 3 个月内没有 RAI;aHR=0.7(0.4-1.1))的女性并非如此。研究结果表明,对 HIV 相关的 RAI 关联进行精确估计,需要对 RAI 暴露进行定义,这一定义仍然存在不完善之处。在研究性行为和 HIV 血清转化时,应更系统、更精确地记录和报告 RAI 实践、RAI/RVI 频率和避孕套使用情况的信息;标准化的措施将有助于跨地域和随时间进行比较。