Nedel Wagner, Deutschendorf Caroline, Portela Luis Valmor Cruz
Intensive Care Unit, Grupo Hospitalar Conceição, Porto Alegre 91350200, Brazil.
Laboratory of Neurotrauma and Biomarkers, Departamento de Bioquímica, ICBS, Universidade Federal do Rio Grande do Sul, Porto Alegre 90035-003, Brazil.
World J Crit Care Med. 2023 Jun 9;12(3):139-152. doi: 10.5492/wjccm.v12.i3.139.
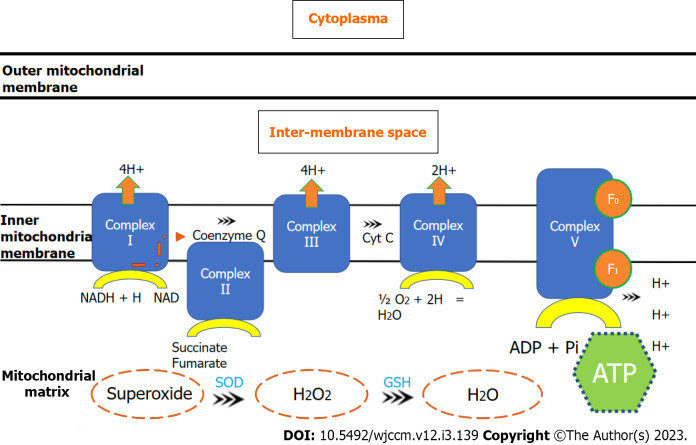
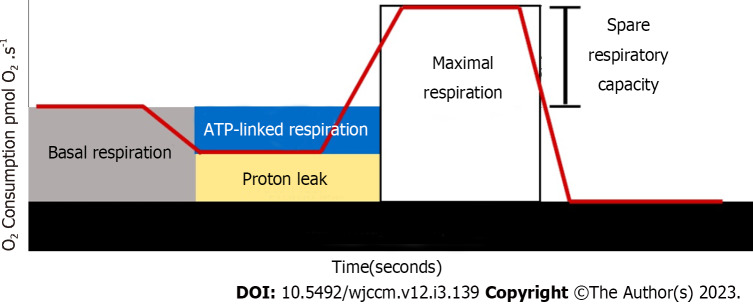
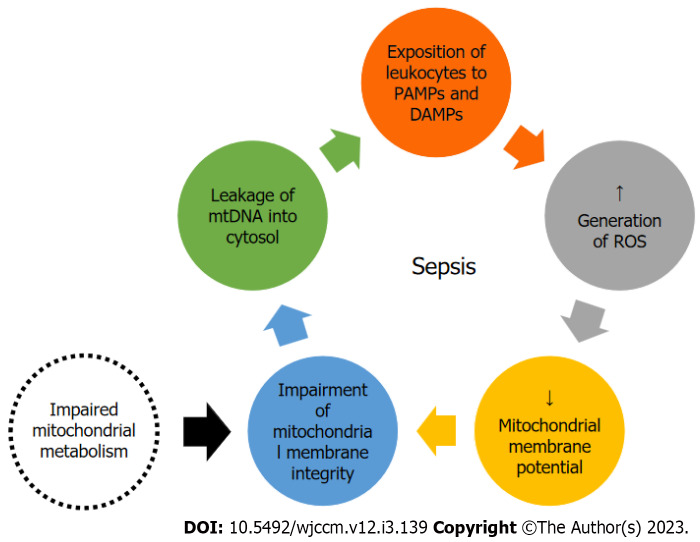
Sepsis represents a deranged and exaggerated systemic inflammatory response to infection and is associated with vascular and metabolic abnormalities that trigger systemic organic dysfunction. Mitochondrial function has been shown to be severely impaired during the early phase of critical illness, with a reduction in biogenesis, increased generation of reactive oxygen species and a decrease in adenosine triphosphate synthesis of up to 50%. Mitochondrial dysfunction can be assessed using mitochondrial DNA concentration and respirometry assays, particularly in peripheral mononuclear cells. Isolation of monocytes and lymphocytes seems to be the most promising strategy for measuring mitochondrial activity in clinical settings because of the ease of collection, sample processing, and clinical relevance of the association between metabolic alterations and deficient immune responses in mononuclear cells. Studies have reported alterations in these variables in patients with sepsis compared with healthy controls and non-septic patients. However, few studies have explored the association between mitochondrial dysfunction in immune mononuclear cells and unfavorable clinical outcomes. An improvement in mitochondrial parameters in sepsis could theoretically serve as a biomarker of clinical recovery and response to oxygen and vasopressor therapies as well as reveal unexplored pathophysiological mechanistic targets. These features highlight the need for further studies on mitochondrial metabolism in immune cells as a feasible tool to evaluate patients in intensive care settings. The evaluation of mitochondrial metabolism is a promising tool for the evaluation and management of critically ill patients, especially those with sepsis. In this article, we explore the pathophysiological aspects, main methods of measurement, and the main studies in this field.
脓毒症是对感染的一种紊乱且过度的全身炎症反应,与引发全身器官功能障碍的血管和代谢异常有关。已表明在危重病早期线粒体功能严重受损,表现为生物合成减少、活性氧生成增加以及三磷酸腺苷合成减少多达50%。线粒体功能障碍可通过线粒体DNA浓度和呼吸测定法进行评估,特别是在外周单核细胞中。由于单核细胞易于采集、样本处理以及代谢改变与单核细胞免疫反应缺陷之间关联的临床相关性,分离单核细胞和淋巴细胞似乎是在临床环境中测量线粒体活性最有前景的策略。与健康对照和非脓毒症患者相比,已有研究报道脓毒症患者这些变量存在改变。然而,很少有研究探讨免疫单核细胞中的线粒体功能障碍与不良临床结局之间的关联。理论上,脓毒症中线粒体参数的改善可作为临床恢复以及对氧疗和血管加压药治疗反应的生物标志物,还能揭示未被探索的病理生理机制靶点。这些特征凸显了进一步研究免疫细胞线粒体代谢作为评估重症监护病房患者可行工具的必要性。线粒体代谢评估是评估和管理危重病患者,尤其是脓毒症患者的一种有前景的工具。在本文中,我们探讨该领域的病理生理学方面、主要测量方法以及主要研究。