Department of Medicine (Hematology-Oncology), University of Pennsylvania, Philadelphia, PA, USA.
Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
Oncologist. 2023 Dec 11;28(12):e1230-e1238. doi: 10.1093/oncolo/oyad183.
Patients with breast cancer in sub-Saharan Africa (SSA) experience a disproportionate burden of mortality. Fidelity to treatment guidelines, defined as receiving optimal dose and frequency of prescribed treatments, improves survival. We sought to identify patient factors associated with treatment fidelity and how this may differ for people with HIV (PWH) and breast cancer.
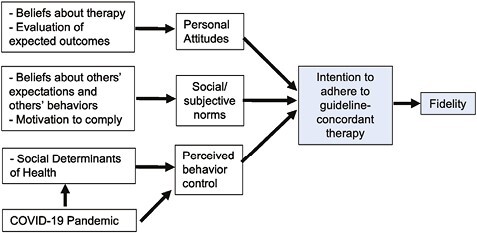
We conducted a qualitative study of women who initiated outpatient treatment for stages I-III breast cancer in Botswana, with deviance sampling of high- and low-fidelity patients. One-on-one interviews were conducted using semi-structured guides informed by the Theory of Planned Behavior. The sample size was determined by thematic saturation. Transcribed interviews were double coded with an integrated analytic approach.
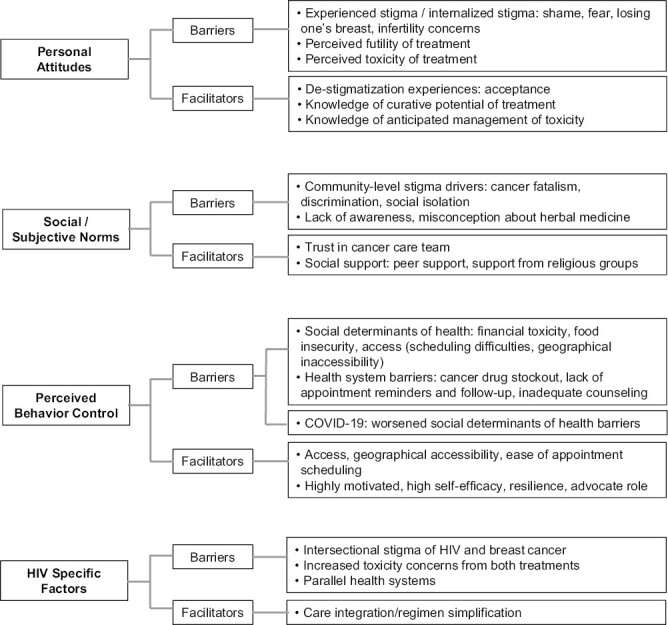
We enrolled 15 high- and 15 low-fidelity participants from August 25, 2020 to December 15, 2020, including 10 PWH (4 high, 6 low fidelity). Ninety-three percent had stage III disease. Barriers to treatment fidelity included stigma, social determinants of health (SDOH), and health system barriers. Acceptance and de-stigmatization, peer and other social support, increased knowledge and self-efficacy were identified as facilitators. The COVID-19 pandemic amplified existing socioeconomic stressors. Unique barriers and facilitators identified by PWH included intersectional stigma, and HIV and cancer care integration, respectively.
We identified multilevel modifiable patient and health system factors associated with fidelity. The facilitators provide opportunities for leveraging existing strengths within the Botswana context to design implementation strategies to increase treatment fidelity to guideline-concordant breast cancer therapy. However, PWH experienced unique barriers, suggesting that interventions to address fidelity may need to be tailored to specific comorbidities.
撒哈拉以南非洲(SSA)的乳腺癌患者面临不成比例的死亡负担。遵循治疗指南(定义为接受最佳剂量和规定治疗的频率)可提高生存率。我们试图确定与治疗一致性相关的患者因素,以及这在 HIV(艾滋病毒)感染者和乳腺癌患者中可能有何不同。
我们对博茨瓦纳接受 I-III 期乳腺癌门诊治疗的女性进行了一项定性研究,对高和低治疗一致性患者进行了偏差抽样。使用基于计划行为理论的半结构化指南进行了一对一访谈。样本量由主题饱和度确定。转录访谈采用综合分析方法进行双编码。
我们于 2020 年 8 月 25 日至 12 月 15 日招募了 15 名高和 15 名低治疗一致性的参与者,包括 10 名 HIV 感染者(4 名高,6 名低)。93%的患者患有 III 期疾病。治疗一致性的障碍包括耻辱感、健康的社会决定因素(SDOH)和卫生系统障碍。接受和去耻辱化、同伴和其他社会支持、增加知识和自我效能感被确定为促进因素。COVID-19 大流行放大了现有的社会经济压力源。艾滋病毒感染者特有的障碍和促进因素分别包括交叉耻辱感和艾滋病毒与癌症护理的整合。
我们确定了与一致性相关的多层次可修改的患者和卫生系统因素。促进因素为利用博茨瓦纳背景下现有的优势提供了机会,以设计实施策略,提高符合指南的乳腺癌治疗的治疗一致性。然而,艾滋病毒感染者经历了独特的障碍,这表明解决一致性的干预措施可能需要针对特定的合并症进行调整。