Demir Muhammed, Özbek Mehmet, Güzel Tuncay, Aktan Adem
Department of Cardiology, Dicle University School of Medicine, Fiskaya Street, Diyarbakir 21280, Turkey.
Department of Cardiology, Health Science University, Gazi Yaşargil Training and Research Hospital, Elazig Street 10. Km Üçkuyular, Kayapınar/Diyarbakır 21070, Turkey.
Eur Heart J Case Rep. 2023 Jul 3;7(7):ytad249. doi: 10.1093/ehjcr/ytad249. eCollection 2023 Jul.
Pheochromocytomas (PHEOs) are a group of tumours that leads to multiple symptoms and can induce hypercoagulability and promote thrombosis. Pheochromocytomas may also present without elevated serum and urinary markers. We aimed to provide tips and tricks for the diagnostic and therapeutic management of an unusual case of PHEOs.
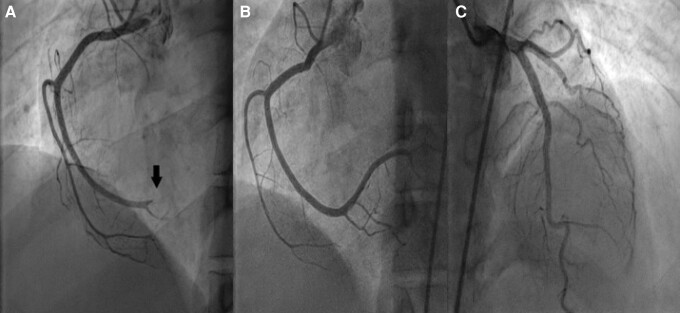
Thirty-four-year-old woman with the unremarkable medical history presented with epigastric pain and dyspnoea. Electrocardiogram showed ST-segment elevation in the inferior limb leads. She underwent an emergency coronary angiogram, which showed a high thrombus burden in the distal right coronary artery. A subsequent echocardiogram demonstrated a 31 × 33 mm right atrial mass adhering to the inferior vena cava and abdominal computed tomography (CT) scan revealed a 113 × 85 mm necrotic mass in the left adrenal bed, with tumour thrombus extending proximally to the confluence of hepatic veins immediately inferior to the right atrium and distally to iliac vein bifurcation. Blood parameters, thrombophilia panel, vanillylmandelic acid, 5 hydroxy indole acetic acid, and homovanillic acid levels were normal. Tissue sampling confirmed the diagnosis of PHEOs. The surgical procedure was not planned due to the presence of metastatic foci on imaging, including positron emission tomography (PET)-CT. Anticoagulation with rivaroxaban and treatment with Lu-DOTATATE-based peptide receptor radionuclide therapy (PRRT) was initiated.
The coexistence of arterial and venous thrombosis is extremely rare in patients with PHEOs. Multidisciplinary approaches are required for the care of such patients. Catecholamines likely contributed to the development of thrombosis in our patient. Early recognition of PHEOs is the key point to ameliorate clinical outcomes.
嗜铬细胞瘤(PHEOs)是一组可导致多种症状并能引起高凝状态和促进血栓形成的肿瘤。嗜铬细胞瘤也可能在血清和尿液标志物未升高的情况下出现。我们旨在为一例不寻常的嗜铬细胞瘤病例的诊断和治疗管理提供技巧和窍门。
一名34岁、病史无异常的女性出现上腹部疼痛和呼吸困难。心电图显示下壁导联ST段抬高。她接受了急诊冠状动脉造影,结果显示右冠状动脉远端血栓负荷较高。随后的超声心动图显示一个31×33毫米的右心房肿块附着于下腔静脉,腹部计算机断层扫描(CT)显示左肾上腺床有一个113×85毫米的坏死肿块,肿瘤血栓近端延伸至右心房下方肝静脉汇合处,远端延伸至髂静脉分叉处。血液参数、血栓形成倾向检测指标、香草扁桃酸、5-羟吲哚乙酸和高香草酸水平均正常。组织活检确诊为嗜铬细胞瘤。由于影像学检查(包括正电子发射断层扫描(PET)-CT)发现有转移灶,未计划进行手术。开始使用利伐沙班进行抗凝治疗,并采用基于镥- DOTATATE的肽受体放射性核素治疗(PRRT)。
嗜铬细胞瘤患者同时存在动脉和静脉血栓形成极为罕见。对此类患者的治疗需要多学科方法。儿茶酚胺可能促成了我们患者血栓的形成。早期识别嗜铬细胞瘤是改善临床结局的关键。