Künstler Erika C S, Bublak Peter, Finke Kathrin, Koranyi Nicolas, Meinhard Marie, Schwab Matthias, Rupprecht Sven
Department of Neurology, Jena University Hospital, Jena, Germany.
Interdisciplinary Centre for Sleep and Ventilatory Medicine, Jena University Hospital, Jena, Germany.
Nat Sci Sleep. 2023 Jun 30;15:491-498. doi: 10.2147/NSS.S399644. eCollection 2023.
Persistent insomnia disorder (pID) is linked to neurocognitive decline and increased risk of Alzheimer's Disease (AD) in later life. However, research in this field often utilizes self-reported sleep quality data - which may be biased by sleep misperception - or uses extensive neurocognitive test batteries - which are often not feasible in clinical settings. This study therefore aims to assess whether a simple screening tool could uncover a specific pattern of cognitive changes in pID patients, and whether these relate to objective aspect(s) of sleep quality.
Neurocognitive performance (Montreal Cognitive Assessment; MoCA), anxiety/depression severity, and subjective sleep quality (Pittsburgh Sleep Quality Index: PSQI; Insomnia Severity Index: ISI) data were collected from 22 middle-aged pID patients and 22 good-sleepers. Patients underwent overnight polysomnography.
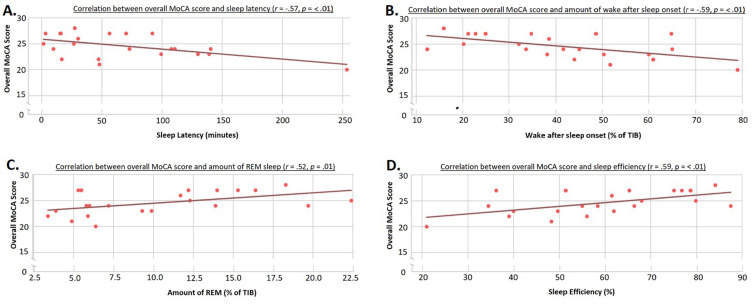
Compared to good-sleepers, patients had lower overall cognitive performance (average: 24.6 versus 26.3 points, Mann-Whitney = 136.5, = <0.006), with deficits in clock drawing and verbal abstraction. In patients, poorer overall cognitive performance correlated with reduced subjective sleep quality (PSQI: (42) = -0.47, = 0.001; and ISI: (42) = -0.43, = 0.004), reduced objective sleep quality (lower sleep efficiency: (20) = 0.59, = 0.004 and less REM-sleep: (20) = 0.52, = 0.013; and increased sleep latency: (20) = -0.57, = 0.005 and time awake: (20) = -0.59, = 0.004). Cognitive performance was not related to anxiety/depression scores.
Using a simple neurocognitive screening tool, we found that pID patients showed cognitive deficiencies that related to both subjective/self-reported and objective/polysomnographic measures of sleep quality. Furthermore, these cognitive changes resembled those seen in preclinical non-amnestic AD, and thus could indicate incumbent neurodegenerative processes in pID. Interestingly, increased REM-sleep was correlated with better cognitive performance. However, whether REM-sleep is protective against neurodegeneration requires further investigation.
持续性失眠障碍(pID)与神经认知功能衰退以及晚年患阿尔茨海默病(AD)的风险增加有关。然而,该领域的研究通常使用自我报告的睡眠质量数据——这可能会因睡眠认知偏差而产生偏差——或者使用大量的神经认知测试组合——这在临床环境中往往不可行。因此,本研究旨在评估一种简单的筛查工具是否能够发现pID患者认知变化的特定模式,以及这些变化是否与睡眠质量的客观方面相关。
收集了22名中年pID患者和22名睡眠良好者的神经认知表现(蒙特利尔认知评估;MoCA)、焦虑/抑郁严重程度以及主观睡眠质量(匹兹堡睡眠质量指数:PSQI;失眠严重程度指数:ISI)数据。患者接受了整夜多导睡眠图检查。
与睡眠良好者相比,患者的整体认知表现较低(平均:24.6分对26.3分,曼-惠特尼U = 136.5,P = <0.006),在画钟试验和语言抽象方面存在缺陷。在患者中,较差的整体认知表现与主观睡眠质量下降相关(PSQI:r(42) = -0.47,P = 0.001;ISI:r(42) = -0.43,P = 0.004),客观睡眠质量下降(睡眠效率较低:r(20) = 0.59,P = 0.004;快速眼动睡眠较少:r(20) = 0.52,P = 0.013;睡眠潜伏期增加:r(20) = -0.57,P = 0.005;清醒时间:r(20) = -0.59,P = 0.004)。认知表现与焦虑/抑郁评分无关。
使用一种简单的神经认知筛查工具,我们发现pID患者存在与睡眠质量的主观/自我报告和客观/多导睡眠图测量均相关的认知缺陷。此外,这些认知变化类似于临床前非遗忘型AD中所见的变化,因此可能表明pID中存在潜在的神经退行性过程。有趣的是,快速眼动睡眠增加与更好的认知表现相关。然而,快速眼动睡眠是否对神经退行性变具有保护作用需要进一步研究。