Department of Geriatric Medicine, Northwest Clinics, Alkmaar, The Netherlands.
Aging and Public Health department, Amsterdam University Medical Centers, Amsterdam, The Netherlands.
BMC Geriatr. 2023 Jul 10;23(1):422. doi: 10.1186/s12877-023-04120-9.
Major bleeding, and intracranial bleeding specifically, are severe complications related to the use of anticoagulation. To what extent the risk for major bleeding is elevated among frail older people is not well known because they are underrepresented in the randomized clinical trials (RCTs). This study investigates the risk for major bleeding (MB) and intra cranial haemorrhage (ICH) in frail older people who fall.
All patients 65 years and older visiting the Fall and Syncope Clinic, between November 2011 and January 2020, and underwent a MRI of the brain were eligible. Frailty was assessed with a Frailty Index, based on the accumulation of deficits model. Cerebral small vessel disease was described and evaluated as proposed in the position paper of Wardlaw and colleagues in 2013.
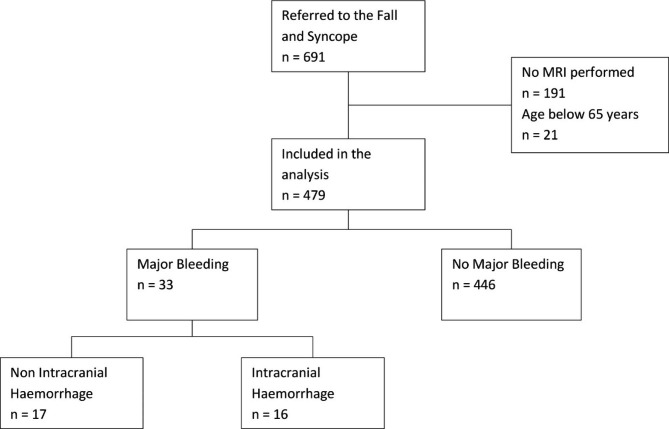
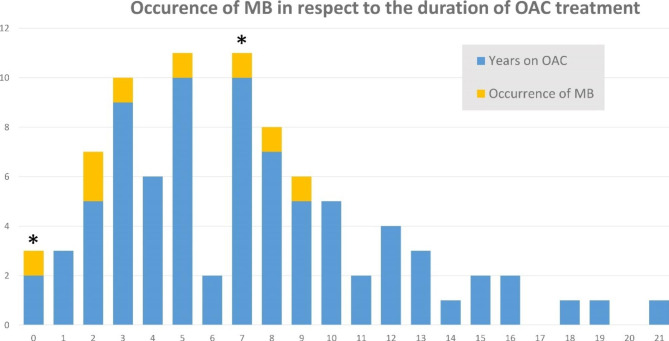
479 patients were included in this analysis. Mean follow-up was 7 years per patient (ranging from 1 month to 8 years and 5 months). 368 patients (77%) were frail. A total of 81 patients used oral anticoagulation (OAC). 17 extracranial MB of which 3 were traumatic and 14 gastrointestinal, and 16 ICH occurred. There was a total of 603.4 treatment years with OAC, and 8 MBs occurred among patients on OAC (bleeding rate 1.32 per 100 treatment years), of which 2 ICHs (bleeding rate 0.33 per 100 treatment years). The risk for extracranial MB was increased by the use of antiplatelet agents (APA) (adjusted OR 6.9, CI 95% 1.2-38.3), and by the use of OAC (adjusted OR 9.8, CI 95% 1.7-56.1). The risk for ICH was only heightened by white matter hyperintensities (WMH) (adjusted OR 3.8, CI 95% 1.0-13.4). The use of APA (adjusted OR 0.9, CI 95% 0.3-3.3) or OAC (adjusted OR 0.6, CI 95% 0.1-3.3) did not elevate the risk for ICH.
In contrast to common belief, frail patients on OAC with repeated falls show a comparable bleeding rate as in the large RCTs, and the use of OAC did not increase the risk for ICH. However, the number of MBs was low, and of ICHs very low, despite extensive follow-up in this registry.
大出血,特别是颅内出血,是与抗凝治疗相关的严重并发症。由于在随机临床试验(RCT)中代表性不足,身体虚弱的老年人发生大出血的风险程度尚不清楚。本研究旨在调查身体虚弱的老年人(≥65 岁)跌倒后发生大出血(MB)和颅内出血(ICH)的风险。
所有于 2011 年 11 月至 2020 年 1 月期间在跌倒和晕厥诊所就诊并接受脑部 MRI 检查的患者均符合条件。采用基于累积缺陷模型的衰弱指数评估衰弱。脑小血管疾病的描述和评估按照 Wardlaw 等人在 2013 年提出的立场文件进行。
本研究共纳入 479 例患者。每位患者的平均随访时间为 7 年(范围为 1 个月至 8 年零 5 个月)。368 例(77%)患者衰弱。共 81 例患者使用口服抗凝药物(OAC)。共发生 17 例颅外 MB,其中 3 例为创伤性,14 例为胃肠道,共发生 16 例 ICH。共发生 603.4 个 OAC 治疗年,接受 OAC 治疗的患者中发生 8 例 MB(出血率为 1.32/100 治疗年),其中 2 例 ICH(出血率为 0.33/100 治疗年)。使用抗血小板药物(APA)(调整后的 OR 6.9,95%CI 1.2-38.3)和使用 OAC(调整后的 OR 9.8,95%CI 1.7-56.1)可增加颅外 MB 的风险。ICH 的风险仅因白质高信号(WMH)(调整后的 OR 3.8,95%CI 1.0-13.4)而增加。使用 APA(调整后的 OR 0.9,95%CI 0.3-3.3)或 OAC(调整后的 OR 0.6,95%CI 0.1-3.3)均不会增加 ICH 的风险。
与普遍看法相反,在反复跌倒的 OAC 治疗的虚弱患者中,出血率与大型 RCT 相当,并且 OAC 的使用并未增加 ICH 的风险。然而,尽管该登记处进行了广泛的随访,但 MB 的数量很少,ICH 的数量非常低。