Department of Anesthesiology, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Hyperbaric Medicine, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, Amsterdam, The Netherlands.
Crit Care. 2023 Jul 12;27(1):282. doi: 10.1186/s13054-023-04563-x.
Iatrogenic cerebral arterial gas embolism (CAGE) caused by invasive medical procedures may be treated with hyperbaric oxygen therapy (HBOT). Previous studies suggested that initiation of HBOT within 6-8 h is associated with higher probability of favorable outcome, when compared to time-to-HBOT beyond 8 h. We performed a group level and individual patient level meta-analysis of observational studies, to evaluate the relationship between time-to-HBOT and outcome after iatrogenic CAGE.
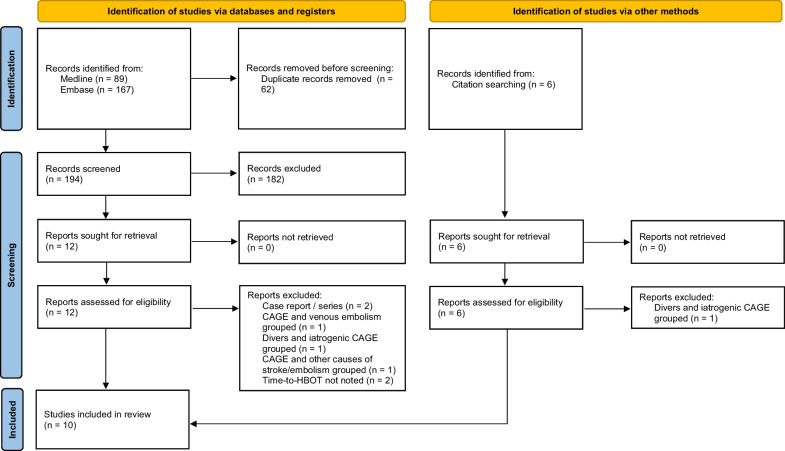
We systematically searched for studies reporting on time-to-HBOT and outcome in patients with iatrogenic CAGE. On group level, we meta-analyzed the differences between median time-to-HBOT in patients with favorable versus unfavorable outcome. On individual patient level, we analyzed the relationship between time-to-HBOT and probability of favorable outcome in a generalized linear mixed effects model.
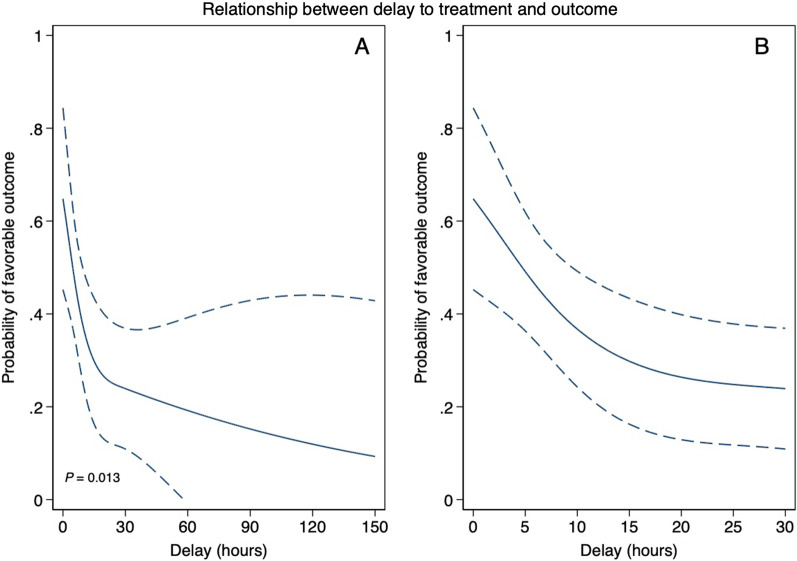
Group level meta-analysis (ten studies, 263 patients) shows that patients with favorable outcome were treated with HBOT 2.4 h (95% CI 0.6-9.7) earlier than patients with unfavorable outcome. The generalized linear mixed effects model (eight studies, 126 patients) shows a significant relationship between time-to-HBOT and probability of favorable outcome (p = 0.013) that remains significant after correcting for severity of manifestations (p = 0.041). Probability of favorable outcome decreases from approximately 65% when HBOT is started immediately, to 30% when HBOT is delayed for 15 h.
Increased time-to-HBOT is associated with decreased probability of favorable outcome in iatrogenic CAGE. This suggests that early initiation of HBOT in iatrogenic CAGE is of vital importance.
由有创医疗操作引起的医源性脑动脉气体栓塞(CAGE)可用高压氧治疗(HBOT)进行治疗。既往研究表明,与 HBOT 时间超过 8 小时相比,6-8 小时内开始 HBOT 与更好的结局概率相关。我们对观察性研究进行了组水平和个体患者水平的荟萃分析,以评估医源性 CAGE 后 HBOT 时间与结局之间的关系。
我们系统地检索了报告医源性 CAGE 患者 HBOT 时间与结局的研究。在组水平上,我们对结局良好与结局不良患者的 HBOT 中位时间进行了荟萃分析。在个体患者水平上,我们在广义线性混合效应模型中分析了 HBOT 时间与良好结局概率之间的关系。
组水平荟萃分析(十项研究,263 例患者)表明,结局良好的患者比结局不良的患者接受 HBOT 治疗早 2.4 小时(95%CI 0.6-9.7)。广义线性混合效应模型(八项研究,126 例患者)显示,HBOT 时间与良好结局概率之间存在显著关系(p=0.013),且在纠正表现严重程度后仍然显著(p=0.041)。当 HBOT 立即开始时,良好结局的概率约为 65%,当 HBOT 延迟 15 小时时,良好结局的概率降至 30%。
HBOT 时间增加与医源性 CAGE 中良好结局的概率降低相关。这表明在医源性 CAGE 中尽早开始 HBOT 至关重要。