Department of Anaesthesiology, University Hospital, LMU Munich, Marchioninistrasse 15, 81377, Munich, Germany.
Department of Anaesthesiology and Intensive Care Medicine, General Hospital of Heidenheim, 89522, Heidenheim, Germany.
Intensive Care Med. 2023 Aug;49(8):966-976. doi: 10.1007/s00134-023-07154-0. Epub 2023 Jul 13.
Inadequate piperacillin (PIP) exposure in intensive care unit (ICU) patients threatens therapeutic success. Model-informed precision dosing (MIPD) might be promising to individualize dosing; however, the transferability of published models to external populations is uncertain. This study aimed to externally evaluate the available PIP population pharmacokinetic (PopPK) models.
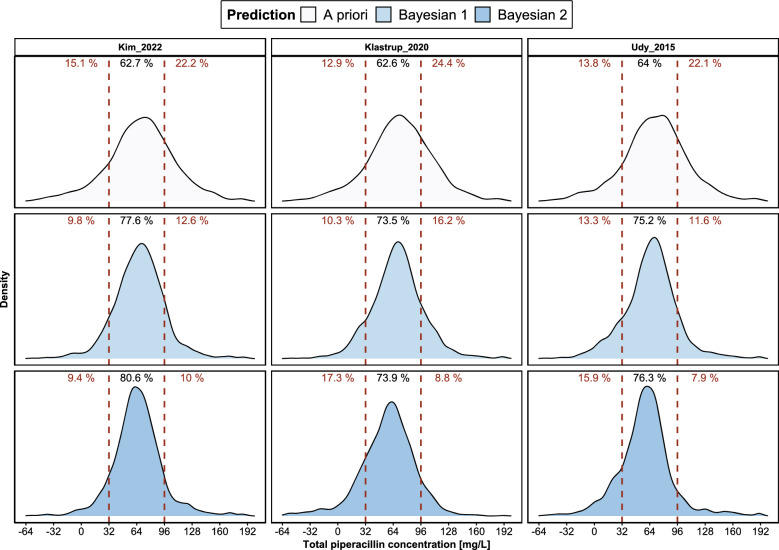
A multicenter dataset of 561 ICU patients (11 centers/3654 concentrations) was used for the evaluation of 24 identified models. Model performance was investigated for a priori (A) predictions, i.e., considering dosing records and patient characteristics only, and for Bayesian forecasting, i.e., additionally including the first (B1) or first and second (B2) therapeutic drug monitoring (TDM) samples per patient. Median relative prediction error (MPE) [%] and median absolute relative prediction error (MAPE) [%] were calculated to quantify accuracy and precision.
The evaluation revealed a large inter-model variability (A: MPE - 135.6-78.3% and MAPE 35.7-135.6%). Integration of TDM data improved all model predictions (B1/B2 relative improvement vs. A: |MPE| 45.1/67.5%; MAPE 29/39%). The model by Kim et al. was identified to be most appropriate for the total dataset (A/B1/B2: MPE - 9.8/- 5.9/- 0.9%; MAPE 37/27.3/23.7%), Udy et al. performed best in patients receiving intermittent infusion, and Klastrup et al. best predicted patients receiving continuous infusion. Additional evaluations stratified by sex and renal replacement therapy revealed further promising models.
The predictive performance of published PIP models in ICU patients varied considerably, highlighting the relevance of appropriate model selection for MIPD. Our differentiated external evaluation identified specific models suitable for clinical use, especially in combination with TDM.
重症监护病房(ICU)患者哌拉西林(PIP)暴露不足会威胁治疗效果。模型指导的精准剂量(MIPD)可能是实现个体化给药的有前途的方法;然而,已发表模型在外部人群中的可转移性尚不确定。本研究旨在对外评估现有的 PIP 群体药代动力学(PopPK)模型。
使用 561 名 ICU 患者(11 个中心/3654 个浓度)的多中心数据集来评估 24 个已确定的模型。通过事先(A)预测,即仅考虑给药记录和患者特征,以及贝叶斯预测(B1 或 B2),即每个患者额外包括第一个(B1)或第一个和第二个(B2)治疗药物监测(TDM)样本,来评估模型性能。计算中位数相对预测误差(MPE)[%]和中位数绝对相对预测误差(MAPE)[%]以量化准确性和精密度。
评估结果显示,模型间存在较大的变异性(A:MPE-135.6-78.3%和 MAPE 35.7-135.6%)。整合 TDM 数据可改善所有模型的预测(B1/B2 与 A 相比的相对改善:|MPE|45.1/67.5%;MAPE 29/39%)。Kim 等人的模型被确定为最适合总数据集的模型(A/B1/B2:MPE-9.8/-5.9/-0.9%;MAPE 37/27.3/23.7%),Udy 等人的模型在接受间歇性输注的患者中表现最佳,而 Klastrup 等人的模型在预测接受连续输注的患者时表现最佳。按性别和肾脏替代治疗进行的进一步评估显示了更有前途的模型。
已发表的 PIP 模型在 ICU 患者中的预测性能差异很大,这凸显了适当模型选择对于 MIPD 的重要性。我们的差异化外部评估确定了特定的适合临床使用的模型,特别是与 TDM 联合使用时。