Coleman Brian C, Lisi Anthony J, Abel Erica A, Runels Tessa, Goulet Joseph L
Pain Research, Informatics, Multimorbidities, and Education (PRIME) Center, VA Connecticut Healthcare System, 950 Campbell Ave, West Haven, CT 06516, United States.
Yale School of Medicine, Yale University, 333 Cedar Street, New Haven, CT 06510, United States.
N Am Spine Soc J. 2023 Jun 1;14:100233. doi: 10.1016/j.xnsj.2023.100233. eCollection 2023 Jun.
Low back pain (LBP) is a common reason individuals seek healthcare. Nonpharmacologic management (NPM) is often recommended as a primary intervention, and earlier use of NPM for LBP shows positive clinical outcomes. Our purpose was to evaluate how timing of engagement in NPM for LBP affects downstream LBP visits during the first year.
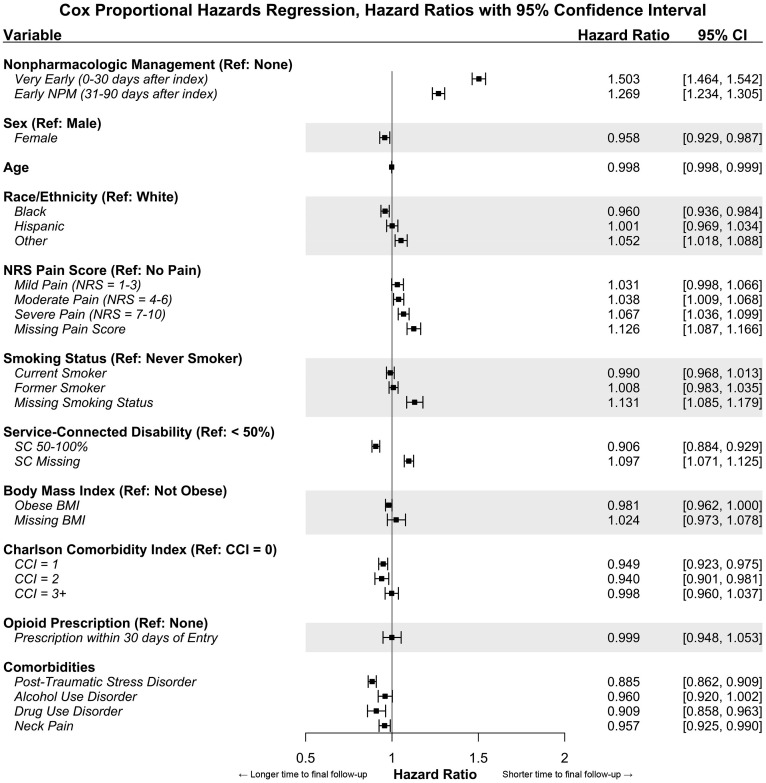
This study was a secondary analysis of an observational cohort study of national electronic health record data. Patients entering the Musculoskeletal Diagnosis/Complementary and Integrative Health Cohort with LBP from October 1, 2016 to September 30, 2017 were included. Exclusive patient groups were defined by engagement in NPM within 30 days of entry ("very early NPM"), between 31 and 90 days ("early NPM"), or not within the first 90 days ("no NPM"). The outcome was time, in days, to the final LBP follow-up after 90 days and within the first year. Cox proportional hazards regression was used to model time to final follow up, controlling for additional demographic and clinical covariables.
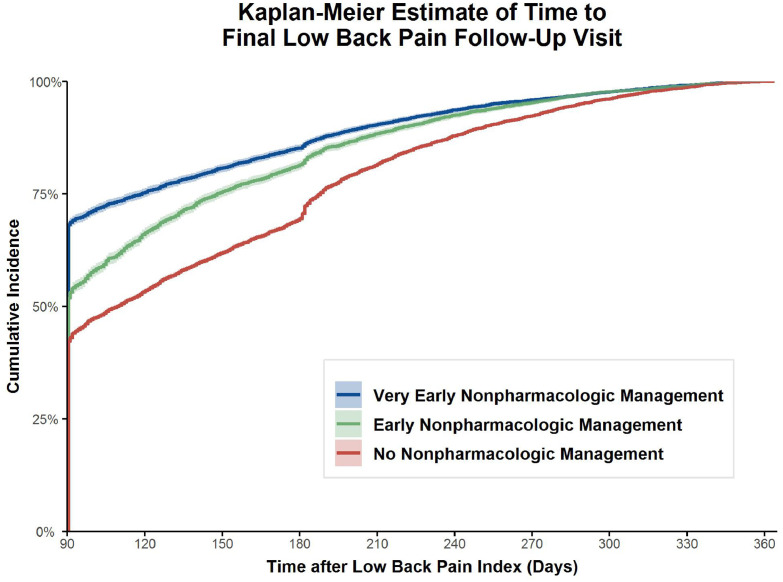
The study population included 44,175 patients, with 16.7% engaging in very early NPM and 13.1% in early NPM. Patients with very early NPM (5.2 visits, SD=4.5) or early NPM (5.7 visits, SD=4.6) had a higher mean number of LBP visits within the first year than those not receiving NPM in the first 90 days (3.2 visits, SD = 2.5). The very early NPM (HR=1.50, 95% CI: 1.46-1.54; median=48 days, IQR=97) and early NPM (HR=1.27, 95% CI: 1.23-1.30; median=88 days, IQR=92) had a significantly shorter time to final follow-up than the no NPM group (median=109 days, IQR=150).
Veterans Health Administration patients receiving NPM for LBP within the first 90 days after initially seeking care demonstrate a significantly faster time to final follow-up visit within the first year compared to those who do not.
腰痛(LBP)是人们寻求医疗保健的常见原因。非药物治疗(NPM)通常被推荐作为主要干预措施,早期对腰痛采用非药物治疗显示出积极的临床效果。我们的目的是评估腰痛非药物治疗的介入时机如何影响第一年期间后续的腰痛就诊情况。
本研究是一项对国家电子健康记录数据进行的观察性队列研究的二次分析。纳入了2016年10月1日至2017年9月30日因腰痛进入肌肉骨骼诊断/补充与综合健康队列的患者。根据在入组后30天内(“极早期NPM”)、31至90天之间(“早期NPM”)或90天内未接受(“无NPM”)非药物治疗来定义不同的患者组。观察指标是90天后及第一年内在最终腰痛随访前的天数。采用Cox比例风险回归模型来分析至最终随访的时间,并控制其他人口统计学和临床协变量。
研究人群包括44175名患者,其中16.7%接受极早期NPM,13.1%接受早期NPM。接受极早期NPM(5.2次就诊,标准差=4.5)或早期NPM(5.7次就诊,标准差=4.6)的患者在第一年的腰痛就诊平均次数高于那些在最初90天内未接受NPM的患者(3.2次就诊,标准差=2.5)。极早期NPM组(风险比=1.50,95%置信区间:1.46 - 1.54;中位数=48天,四分位距=97)和早期NPM组(风险比=1.27,95%置信区间:1.23 - 1.30;中位数=88天,四分位距=92)至最终随访的时间显著短于无NPM组(中位数=109天,四分位距=150)。
与未接受非药物治疗的患者相比,在最初寻求治疗后的前90天内接受腰痛非药物治疗的退伍军人健康管理局患者在第一年至最终随访就诊的时间明显更快。