Mohile Neil V, Kuczmarski Alexander S, Minaie Arya, Syros Alina, Geller Joseph S, Maaieh Motasem Al
Department of Orthopaedic Surgery, Jackson Memorial Hospital, University of Miami Health System, 1611 NW 12th Ave, Miami, FL 33136, United States.
Department of Medical Education, University of Miami Miller School of Medicine, 1600 NW 10th Ave #1140, Miami, FL 33136, United States.
N Am Spine Soc J. 2023 Apr 24;14:100224. doi: 10.1016/j.xnsj.2023.100224. eCollection 2023 Jun.
Combined atlas-axis fractures are rare occurrences with substantially higher rates of neurologic deficits compared with isolated injuries. Given the intricate anatomic relationship between the atlas and axis vertebra, variable fracture patterns may occur, warranting special considerations from surgeons.
A systematic search of PubMed and EMBASE was performed following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. Relevant studies on acute combined atlas-axis fractures that provided data on patient demographics, presentation (injury mechanism, neurologic deficits, fracture type), management, complications, and study conclusions were reviewed.
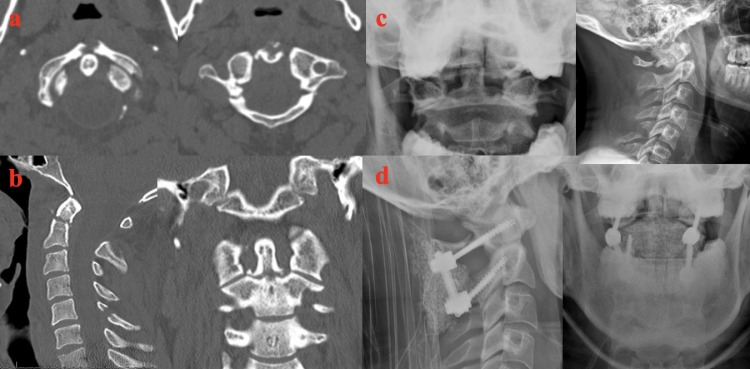
A total of 22 articles published from 1977 to 2022, comprising 230 patients, were included in the final analysis. Thirty-seven of the 213 patients (17%) presented with neurologic deficits. The most common atlas injuries were posterior arch fractures (54/169 patients; 32%), combined posterior arch/anterior arch fractures (44/169 patients; 26%), and anterior arch fractures (43/169 patients; 25%). The most common axis injuries were type II odontoid fractures (115/175 patients; 66%). Of the 127 patients managed operatively (127/230 patients; 55%), 45 patients (35%) were treated with C1-C2 posterior spinal fusion, 33 patients (26%) were treated with odontoid screw fixation and anterior/posterior C1-C2 trans-articular screws, 16 patients (13%) were treated with occiputocervical fusion and 12 patients (9%) were treated with odontoid screw fixation alone.
Management strategies are generally based on the type of axis fracture as well as the condition of the transverse ligament. Patients with stable fractures can be successfully managed nonoperatively with a cervical collar or halo immobilization. Combined atlas-axis fractures with an atlantodental interval >5 mm, C1 lateral mass displacement >7 mm, C2-C3 angulation >11° or an MRI demonstrating a disrupted transverse ligament are suggestive of instability and are often successfully managed with surgical intervention. There is no consensus regarding surgical technique.
寰枢椎联合骨折较为罕见,与单纯损伤相比,神经功能缺损发生率显著更高。鉴于寰椎与枢椎之间复杂的解剖关系,可能会出现多种骨折类型,这需要外科医生特别关注。
按照系统评价和Meta分析的首选报告项目(PRISMA)指南,对PubMed和EMBASE进行系统检索。对有关急性寰枢椎联合骨折的相关研究进行综述,这些研究提供了患者人口统计学、表现(损伤机制、神经功能缺损、骨折类型)、治疗、并发症及研究结论等方面的数据。
最终分析纳入了1977年至2022年发表的共22篇文章,包含230例患者。213例患者中有37例(17%)出现神经功能缺损。最常见的寰椎损伤为后弓骨折(54/169例患者;32%)、后弓/前弓联合骨折(44/169例患者;26%)和前弓骨折(43/169例患者;25%)。最常见的枢椎损伤为Ⅱ型齿状突骨折(115/175例患者;66%)。在127例接受手术治疗的患者中(127/230例患者;55%),45例患者(35%)接受了C1-C2后路脊柱融合术,33例患者(26%)接受了齿状突螺钉固定及C1-C2前后路经关节螺钉固定,16例患者(13%)接受了枕颈融合术,12例患者(9%)仅接受了齿状突螺钉固定。
治疗策略通常基于枢椎骨折类型以及横韧带的情况。稳定骨折患者通过颈托或头环固定可成功进行非手术治疗。寰枢椎联合骨折患者若寰齿间距>5 mm、C1侧块移位>7 mm、C2-C3成角>11°或MRI显示横韧带断裂,则提示不稳定,通常通过手术干预可成功治疗。关于手术技术尚无共识。