Chifotides Helen T, Verstovsek Srdan, Bose Prithviraj
Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA.
Cancers (Basel). 2023 Jun 24;15(13):3331. doi: 10.3390/cancers15133331.
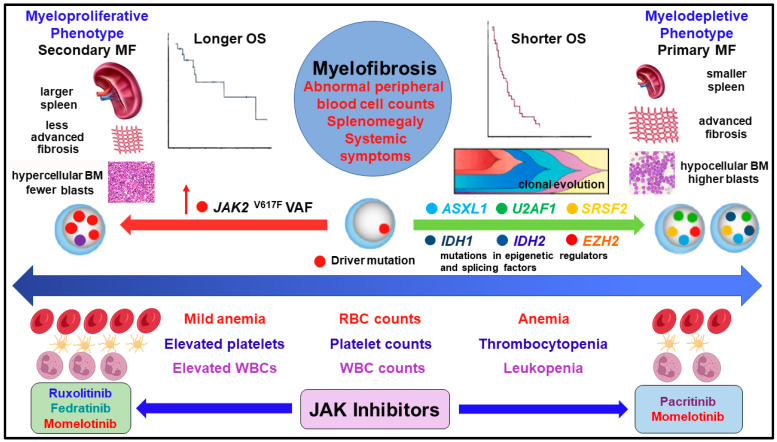
Myelofibrosis (MF) presents an array of clinical manifestations and molecular profiles. The two distinct phenotypes- myeloproliferative and myelodepletive or cytopenic- are situated at the two poles of the disease spectrum and are largely defined by different degrees of cytopenias, splenomegaly, and distinct molecular profiles. The myeloproliferative phenotype is characterized by normal/higher peripheral blood counts or mildly decreased hemoglobin, progressive splenomegaly, and constitutional symptoms. The myeloproliferative phenotype is typically associated with secondary MF, higher V617F burden, fewer mutations, and superior overall survival (OS). The myelodepletive phenotype is usually associated with primary MF, ≥2 cytopenias, modest splenomegaly, lower V617F burden, higher fibrosis, greater genomic complexity, and inferior OS. Cytopenias are associated with mutations in epigenetic regulators/splicing factors, clonal evolution, disease progression, and shorter OS. Clinical variables, in conjunction with the molecular profiles, inform integrated prognostication and disease management. Ruxolitinib/fedratinib and pacritinib/momelotinib may be more suitable to treat patients with the myeloproliferative and myelodepletive phenotypes, respectively. Appreciation of MF heterogeneity and two distinct phenotypes, the different clinical manifestations and molecular profiles associated with each phenotype alongside the growing treatment expertise, the development of non-myelosuppressive JAK inhibitors, and integrated prognostication are leading to a new era in patient management. Physicians can increasingly tailor personalized treatments that will address the unique unmet needs of MF patients, including those presenting with the myelodepletive phenotype, to elicit optimal outcomes and extended OS across the disease spectrum.
骨髓纤维化(MF)呈现出一系列临床表现和分子特征。两种不同的表型——骨髓增殖型和骨髓消耗型或血细胞减少型——位于疾病谱的两极,主要由不同程度的血细胞减少、脾肿大和不同的分子特征来界定。骨髓增殖型表型的特征是外周血细胞计数正常/升高或血红蛋白轻度降低、进行性脾肿大和全身症状。骨髓增殖型表型通常与继发性MF、较高的V617F负荷、较少的突变以及较好的总生存期(OS)相关。骨髓消耗型表型通常与原发性MF、≥2种血细胞减少、轻度脾肿大、较低的V617F负荷、较高的纤维化、更高的基因组复杂性以及较差的OS相关。血细胞减少与表观遗传调节因子/剪接因子的突变、克隆进化、疾病进展和较短的OS相关。临床变量与分子特征相结合,有助于进行综合预后评估和疾病管理。鲁索替尼/费拉替尼和帕西替尼/莫美替尼可能分别更适合治疗骨髓增殖型和骨髓消耗型表型的患者。对MF异质性和两种不同表型的认识、与每种表型相关的不同临床表现和分子特征、不断增长的治疗专业知识、非骨髓抑制性JAK抑制剂的开发以及综合预后评估,正引领着患者管理的新时代。医生能够越来越多地定制个性化治疗方案,以满足MF患者独特的未满足需求,包括那些表现为骨髓消耗型表型的患者,从而在整个疾病谱中获得最佳疗效和延长OS。