Gavriilaki Eleni, Dolgyras Panagiotis, Dimou-Mpesikli Sotiria, Poulopoulou Aikaterini, Evangelidis Paschalis, Evangelidis Nikolaos, Demosthenous Christos, Zachrou Evangelia, Siasios Panagiotis, Mallouri Despina, Vardi Anna, Bousiou Zoi, Panteliadou Alkistis, Batsis Ioannis, Masmanidou Marianna, Lalayanni Chrysavgi, Yannaki Evangelia, Sotiropoulos Damianos, Anagnostopoulos Achilles, Vyzantiadis Timoleon-Achilleas, Sakellari Ioanna
Bone Marrow Transplantation Unit, Haematology Department, G. Papanicolaou Hospital, 57010 Thessaloniki, Greece.
Second Propedeutic Department of Internal Medicine, Hippocration Hospital, Aristotle University of Thessaloniki, 54642 Thessaloniki, Greece.
Cancers (Basel). 2023 Jul 7;15(13):3529. doi: 10.3390/cancers15133529.
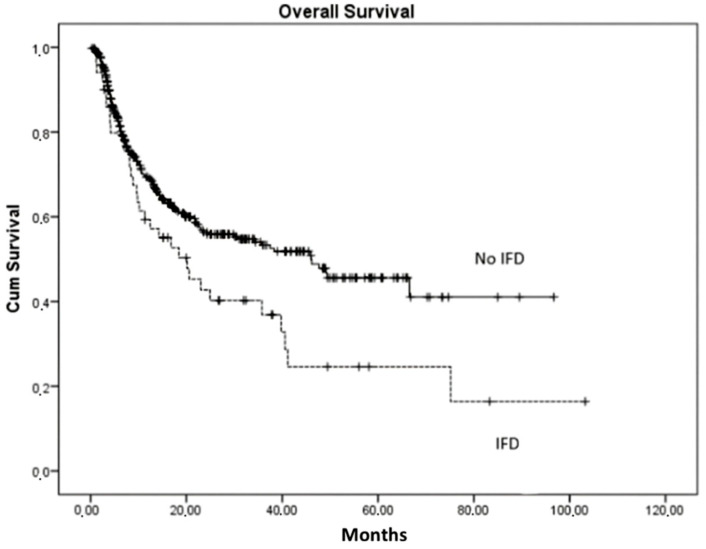
(1) Background: Autologous, allogeneic hematopoietic cell transplantation (HCT) and other cellular therapies, including CAR T cell and gene therapy, constitute a cornerstone in the management of various benign and malignant hematological disorders. Invasive fungal infections (IFD) remain a significant cause of morbidity and mortality in HCT recipients. Therefore, we investigated the prevalence and risk factors of IFD following HCT and other cellular therapies in an era of novel antifungal prophylaxis. (2) Methods: In this study, we retrospectively enrolled adult HCT recipients who were treated at our JACIE-accredited center according to standard operating procedures over the last decade (2013-2022). (3) Results: 950 patients who received cellular therapies were studied. None of the 19 CAR T cell and neither of the two gene therapy recipients developed IFD whereas 3/456 autologous HCT recipients who suffered from primary refractory/relapsed lymphomas presented with probable IFD. Overall, 11 patients who received allogeneic HCT experienced probable IFD, possible IFD was found in 31/473, and IFD was proven in 10/473. A second IFD episode was present in three patients. Four-year OS was significantly lower in proven compared to probable IFD ( = 0.041) and was independently associated with HCT-CI ( = 0.040) and chronic GVHD ( = 0.045). (4) Conclusions: In this real-world cohort, the prevalence of proven and probable IFD in an era of novel antifungal prophylaxis was found to be relatively low. However, IFDs were associated with poor outcomes for patients who received allogeneic HCT.
(1)背景:自体、异体造血细胞移植(HCT)以及其他细胞疗法,包括嵌合抗原受体(CAR)T细胞疗法和基因疗法,是治疗各种良性和恶性血液系统疾病的基石。侵袭性真菌感染(IFD)仍然是HCT受者发病和死亡的重要原因。因此,我们在新型抗真菌预防时代,研究了HCT及其他细胞疗法后IFD的患病率和危险因素。(2)方法:在本研究中,我们回顾性纳入了过去十年(2013 - 2022年)在我们经国际细胞治疗认证基金会(JACIE)认可的中心按照标准操作程序接受治疗的成年HCT受者。(3)结果:对950例接受细胞疗法的患者进行了研究。19例接受CAR T细胞疗法的患者和2例接受基因疗法的患者均未发生IFD,而456例患有原发性难治性/复发性淋巴瘤的自体HCT受者中有3例出现可能的IFD。总体而言,11例接受异体HCT的患者出现可能的IFD,在473例中有31例发现可能的IFD,在473例中有10例确诊为IFD。3例患者出现第二次IFD发作。确诊IFD患者的4年总生存率显著低于可能发生IFD的患者(P = 0.041),并且与造血细胞移植合并症指数(HCT - CI,P = 0.040)和慢性移植物抗宿主病(GVHD,P = 0.045)独立相关。(4)结论:在这个真实世界队列中,发现在新型抗真菌预防时代确诊和可能的IFD患病率相对较低。然而,IFD与接受异体HCT的患者的不良预后相关。