Bancke Laverde Bruno Leonardo, Maak Matthias, Langheinrich Melanie, Kersting Stephan, Denz Axel, Krautz Christian, Weber Georg F, Grützmann Robert, Brunner Maximilian
Department of General and Visceral Surgery, Friedrich-Alexander-University, Krankenhausstraße 12, 91054 Erlangen, Germany.
Department of General, Visceral, Thoracic and Vascular Surgery, University Greifswald, Ferdinand-Sauerbruch-Straße, 17475 Greifswald, Germany.
J Clin Med. 2023 Jun 27;12(13):4299. doi: 10.3390/jcm12134299.
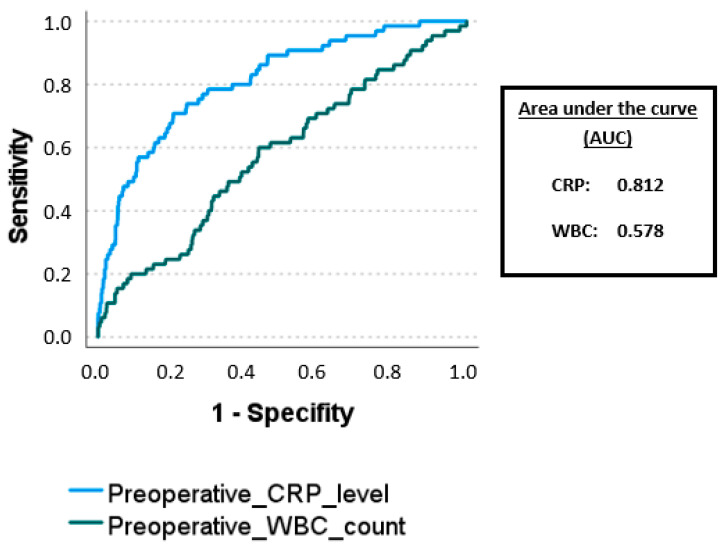
(1) Background: Since its introduction in the 1990s, laparoscopic appendectomy has become established over the years and is today considered the standard therapy for acute appendicitis. In some cases, however, a conversion to the open approach is still necessary. The primary aim of this study was to identify risk factors for the need to convert from the laparoscopic to an open approach during appendectomy for acute appendicitis. (2) Methods: A retrospective analysis of 1220 adult patients who underwent laparoscopic appendectomy for acute appendicitis from 2010 to 2020 at the University Hospital Erlangen was performed. Data, including patient demographics and pre-, intra-, and postoperative findings, were collected and compared between patients with and without conversion. (3) Results: The conversion rate in our cohort was 5.5%. A higher preoperative WBC count and CRP (OR 1.9, = 0.042, and OR 2.3, = 0.019, respectively), as well as the presence of intraoperative perforation, necrosis or gangrene, perityphlitic abscess and peritonitis (OR 3.2, = 0.001; OR 2.3, = 0.023; OR 2.6, = 0.006 and OR 2.0, = 0.025, respectively) were identified as independent risk factors for conversion from the laparoscopic to the open approach. Conversion was again independently associated with higher morbidity (OR 2.2, = 0.043). (4) Conclusion: The laparoscopic approach is feasible and safe in the majority of patients with acute appendicitis. Only increased inflammatory blood markers could be detected as the preoperative risk factors potentially influencing the choice of surgical approach but only with low specificity and sensitivity. For the decision to convert, intraoperative findings are additionally crucial. However, patients with conversion should receive special attention in the postoperative course, as these have an increased risk of developing complications.
(1) 背景:自20世纪90年代引入以来,腹腔镜阑尾切除术多年来已得到确立,如今被视为急性阑尾炎的标准治疗方法。然而,在某些情况下,仍有必要转为开放手术。本研究的主要目的是确定急性阑尾炎阑尾切除术中从腹腔镜手术转为开放手术的危险因素。(2) 方法:对2010年至2020年在埃尔朗根大学医院接受腹腔镜阑尾切除术治疗急性阑尾炎的1220例成年患者进行回顾性分析。收集包括患者人口统计学资料以及术前、术中和术后检查结果的数据,并在有和没有转为开放手术的患者之间进行比较。(3) 结果:我们队列中的中转率为5.5%。术前白细胞计数和C反应蛋白升高(分别为OR 1.9,P = 0.042;OR 2.3,P = 0.019),以及术中存在穿孔、坏死或坏疽、盲肠周围脓肿和腹膜炎(分别为OR 3.2,P = 0.001;OR 2.3,P = 0.023;OR 2.6,P = 0.006;OR 2.0,P = 0.025)被确定为从腹腔镜手术转为开放手术的独立危险因素。中转再次与更高的发病率独立相关(OR 2.2,P = 0.043)。(4) 结论:腹腔镜手术方法在大多数急性阑尾炎患者中是可行且安全的。仅炎症血液标志物升高可被检测为可能影响手术方法选择的术前危险因素,但特异性和敏感性均较低。对于中转的决定,术中发现同样至关重要。然而,中转患者在术后过程中应受到特别关注,因为这些患者发生并发症的风险增加。