Department of Obstetrics and Gynecology, La Conception Hospital, Assistance Publique-Hopitaux de Marseille, Marseille, France.
Aix-Marseille Univ, IRD, Assistance Publique-Hopitaux de Marseille, UMRD-258 Microbes, Evolution, Phylogenie and Infection (MEPHI), Marseille, France.
JAMA Pediatr. 2023 Sep 1;177(9):894-902. doi: 10.1001/jamapediatrics.2023.2250.
Bacterial vaginosis (BV) is a well-known risk factor for preterm birth. Molecular diagnosis of BV is now available. Its impact in the screening and treatment of BV during pregnancy on preterm births has not been evaluated to date.
To evaluate the clinical and economic effects of point-of-care quantitative real-time polymerase chain reaction screen and treat for BV in low-risk pregnant women on preterm birth.
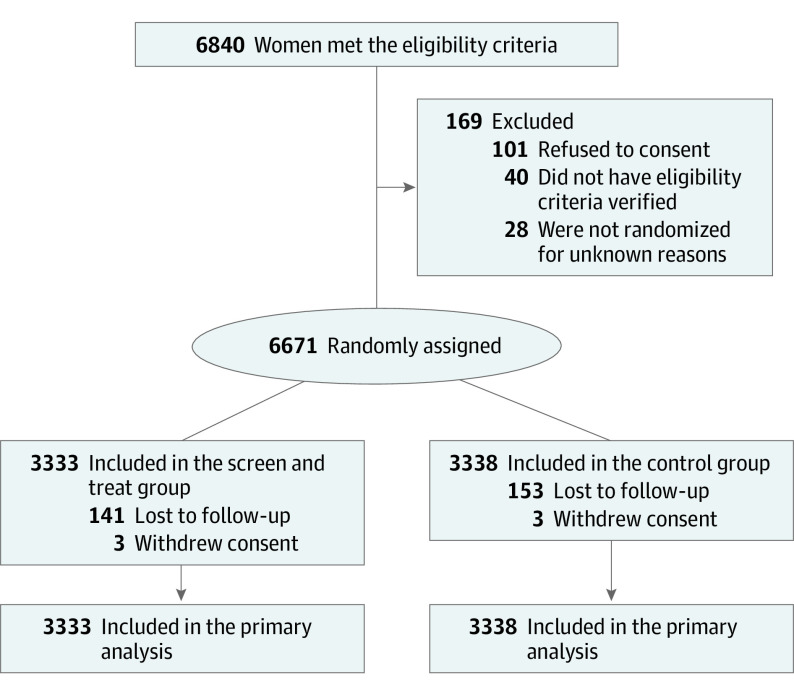
DESIGN, SETTING, AND PARTICIPANTS: The AuTop trial was a prospective, multicenter, parallel, individually randomized, open-label, superiority trial conducted in 19 French perinatal centers between March 9, 2015, and December 18, 2017. Low-risk pregnant women before 20 weeks' gestation without previous preterm births or late miscarriages were enrolled. Data were analyzed from October 2021 to November 2022.
Participants were randomized 1:1 to BV screen and treat using self-collected vaginal swabs (n = 3333) or usual care (n = 3338). BV was defined as Atopobium vaginae (Fannyhessea vaginae) load of 108 copies/mL or greater and/or Gardnerella vaginalis load of 109 copies/mL or greater, using point-of-care quantitative real-time polymerase chain reaction assays. The control group received usual care with no screening of BV.
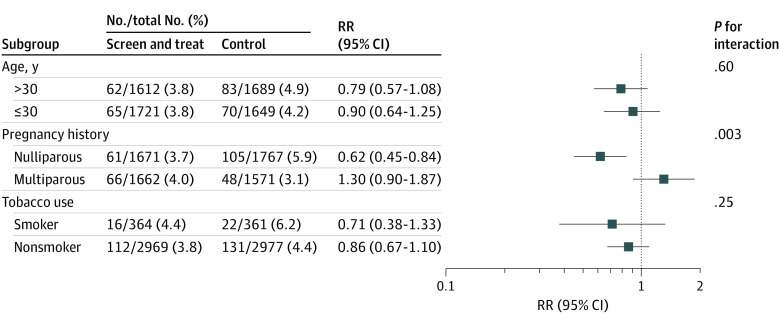
Overall rate of preterm birth before 37 weeks' gestation and total costs were calculated in both groups. Secondary outcomes were related to treatment success as well as maternal and neonate health. Post hoc subgroup analyses were conducted.
Among 6671 randomized women (mean [SD] age, 30.6 [5.0] years; mean [SD] gestational age, 15.5 [2.8] weeks), the intention-to-treat analysis of the primary clinical and economic outcomes showed no evidence of a reduction in the rate of preterm birth and total costs with the screen and treat strategy compared with usual care. The rate of preterm birth was 3.8% (127 of 3333) in the screen and treat group and 4.6% (153 of 3338) in the control group (risk ratio [RR], 0.83; 95% CI, 0.66-1.05; P = .12). On average, the cost of the intervention was €203.6 (US $218.0) per participant, and the total average cost was €3344.3 (US $3580.5) in the screen and treat group vs €3272.9 (US $3504.1) in the control group, with no significant differences being observed. In the subgroup of nulliparous women (n = 3438), screen and treat was significantly more effective than usual care (RR, 0.62; 95% CI, 0.45-0.84; P for interaction = .003), whereas no statistical difference was found in multiparous (RR, 1.30; 95% CI, 0.90-1.87).
In this clinical trial of pregnant women at low risk of preterm birth, molecular screening and treatment for BV based on A vaginae (F vaginae) and/or G vaginalis quantification did not significantly reduce preterm birth rates. Post hoc analysis suggests a benefit of screen and treat in low-risk nulliparous women, warranting further evaluation in this group.
ClinicalTrials.gov Identifier: NCT02288832.
细菌性阴道病(BV)是早产的已知危险因素。现在可以进行分子诊断BV。尚未评估其在妊娠期间对 BV 的筛查和治疗对早产的影响。
评估在低危孕妇中进行即时定量实时聚合酶链反应(PCR)筛查和治疗 BV 对早产的临床和经济影响。
设计、地点和参与者:AuTop 试验是一项前瞻性、多中心、平行、个体随机、开放性、优效性试验,于 2015 年 3 月 9 日至 2017 年 12 月 18 日在 19 个法国围产期中心进行。招募的是在 20 周妊娠前无早产史或晚期流产史的低危孕妇。数据分析于 2021 年 10 月至 2022 年 11 月进行。
参与者以 1:1 的比例随机分为使用自我采集的阴道拭子(n=3333)或常规护理(n=3338)的 BV 筛查和治疗组。使用即时定量 PCR 检测,BV 定义为 Atopobium vaginae(Fannyhessea vaginae)负荷量为 108 拷贝/ml 或更高和/或 Gardnerella vaginalis 负荷量为 109 拷贝/ml 或更高。对照组接受常规护理,不筛查 BV。
计算两组的总早产率和总费用。次要结局与治疗成功率以及母婴健康有关。进行了事后亚组分析。
在 6671 名随机分配的女性(平均[标准差]年龄,30.6[5.0]岁;平均[标准差]妊娠周数,15.5[2.8]周)中,意向治疗分析的主要临床和经济结局显示,与常规护理相比,筛查和治疗策略并没有降低早产率和总费用。筛查和治疗组的早产率为 3.8%(127/3333),对照组为 4.6%(153/3338)(风险比[RR],0.83;95%置信区间[CI],0.66-1.05;P=0.12)。平均而言,干预的费用为每位参与者 203.6 欧元(218.0 美元),筛查和治疗组的总平均费用为 3344.3 欧元(3580.5 美元),对照组为 3272.9 欧元(3504.1 美元),无显著差异。在未产妇(n=3438)亚组中,筛查和治疗明显优于常规护理(RR,0.62;95%CI,0.45-0.84;P 交互=0.003),而在多产妇(RR,1.30;95%CI,0.90-1.87)中未发现统计学差异。
在这项针对低危早产风险孕妇的临床试验中,基于 A vaginae(F vaginae)和/或 G vaginalis 定量的分子筛查和治疗并没有显著降低早产率。事后分析表明,筛查和治疗对低危未产妇有益,值得在该人群中进一步评估。
ClinicalTrials.gov 标识符:NCT02288832。