Institute of Human Genetics, University of Leipzig Medical Center, Leipzig, 04103, Germany.
Berlin Institute of Health at Charité - Universitätsmedizin Berlin, Center of Functional Genomics, Hessische Straße 4A, 10115, Berlin, Germany.
Eur J Hum Genet. 2023 Oct;31(10):1154-1164. doi: 10.1038/s41431-023-01425-6. Epub 2023 Jul 18.
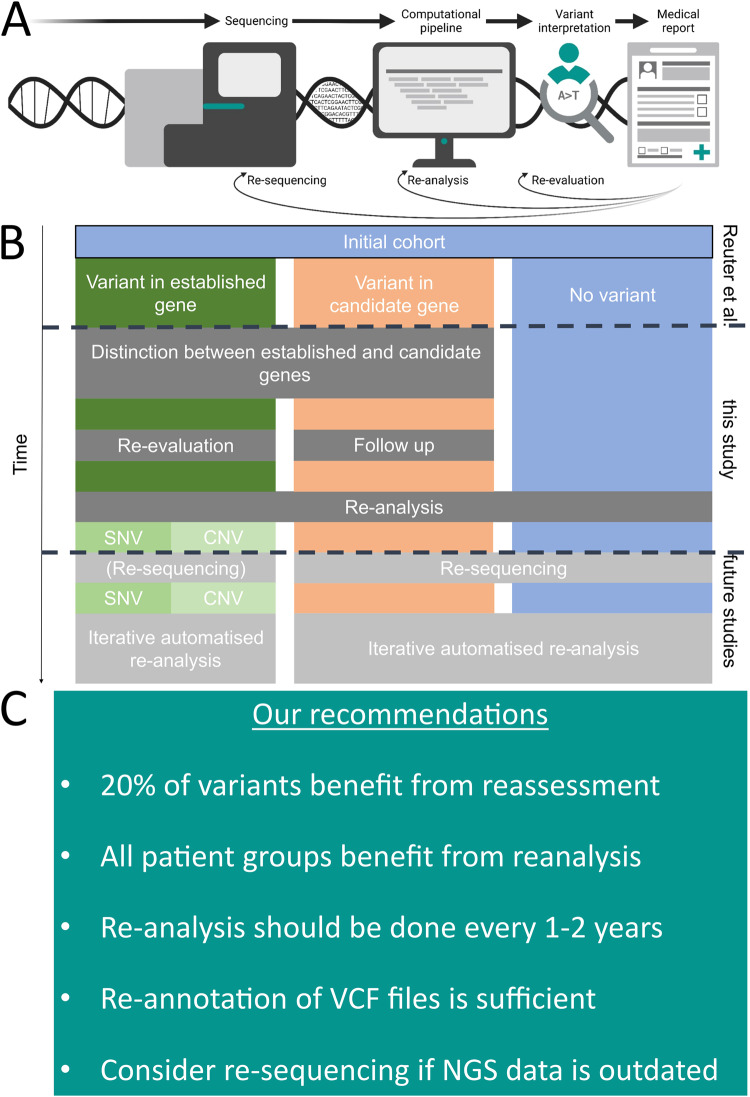
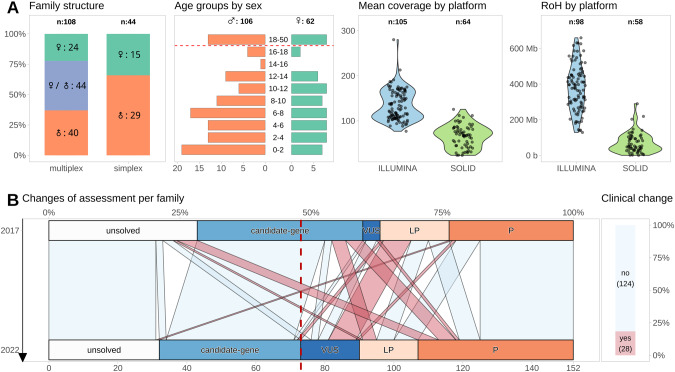
Iterative re-analysis of NGS results is not well investigated for published research cohorts of rare diseases. We revisited a cohort of 152 consanguineous families with developmental disorders (NDD) reported five years ago. We re-evaluated all reported variants according to diagnostic classification guidelines or our candidate gene scoring system (AutoCaSc) and systematically scored the validity of gene-disease associations (GDA). Sequencing data was re-processed using an up-to-date pipeline for case-level re-analysis. In 28/152 (18%) families, we identified a clinically relevant change. Ten previously reported (likely) pathogenic variants were re-classified as VUS/benign. In one case, the GDA (TSEN15) validity was judged as limited, and in five cases GDAs are meanwhile established. We identified 12 new disease causing variants. Two previously reported variants were missed by our updated pipeline due to alignment or reference issues. Our results support the need to re-evaluate screening studies, not only the negative cases but including supposedly solved ones. This also applies in a diagnostic setting. We highlight that the complexity of computational re-analysis for old data should be weighed against the decreasing re-testing costs. Since extensive re-analysis per case is beyond the resources of most institutions, we recommend a screening procedure that would quickly identify the majority (83%) of new variants.
对于已发表的罕见病研究队列,迭代重新分析 NGS 结果的研究并不多。我们重新研究了五年前报道的 152 个有发育障碍(NDD)的近亲家庭队列。我们根据诊断分类指南或我们的候选基因评分系统(AutoCaSc)重新评估了所有报告的变异,并系统地评估了基因疾病关联(GDA)的有效性。使用最新的病例级重新分析管道重新处理测序数据。在 28/152(18%)个家庭中,我们发现了一个具有临床相关性的变化。10 个先前报告的(可能)致病性变异被重新分类为 VUS/良性。在一个病例中,GDA(TSEN15)的有效性被判断为有限,同时在五个病例中建立了 GDA。我们鉴定了 12 个新的致病变异。由于比对或参考问题,我们的更新管道错过了两个先前报告的变异。我们的结果支持重新评估筛选研究的必要性,不仅包括阴性病例,还包括那些据称已解决的病例。这在诊断环境中也是如此。我们强调,对旧数据进行复杂的计算重新分析,应该权衡重新测试成本的降低。由于每个病例的广泛重新分析超出了大多数机构的资源能力,因此我们建议采用一种筛选程序,该程序可以快速识别大多数(83%)新变异。