Department of Health Sciences, University of Florence, Florence, Italy.
Pediatric Unit, Meyer Children's Hospital IRCCS, Viale Pieraccini 24, Florence, 50139, Italy.
Eur J Pediatr. 2023 Oct;182(10):4341-4349. doi: 10.1007/s00431-023-05115-9. Epub 2023 Jul 18.
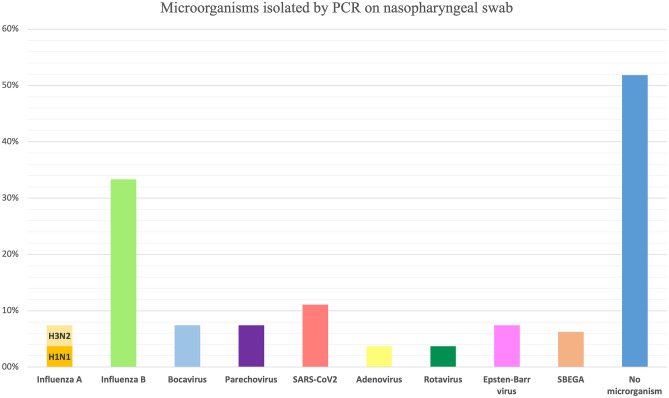
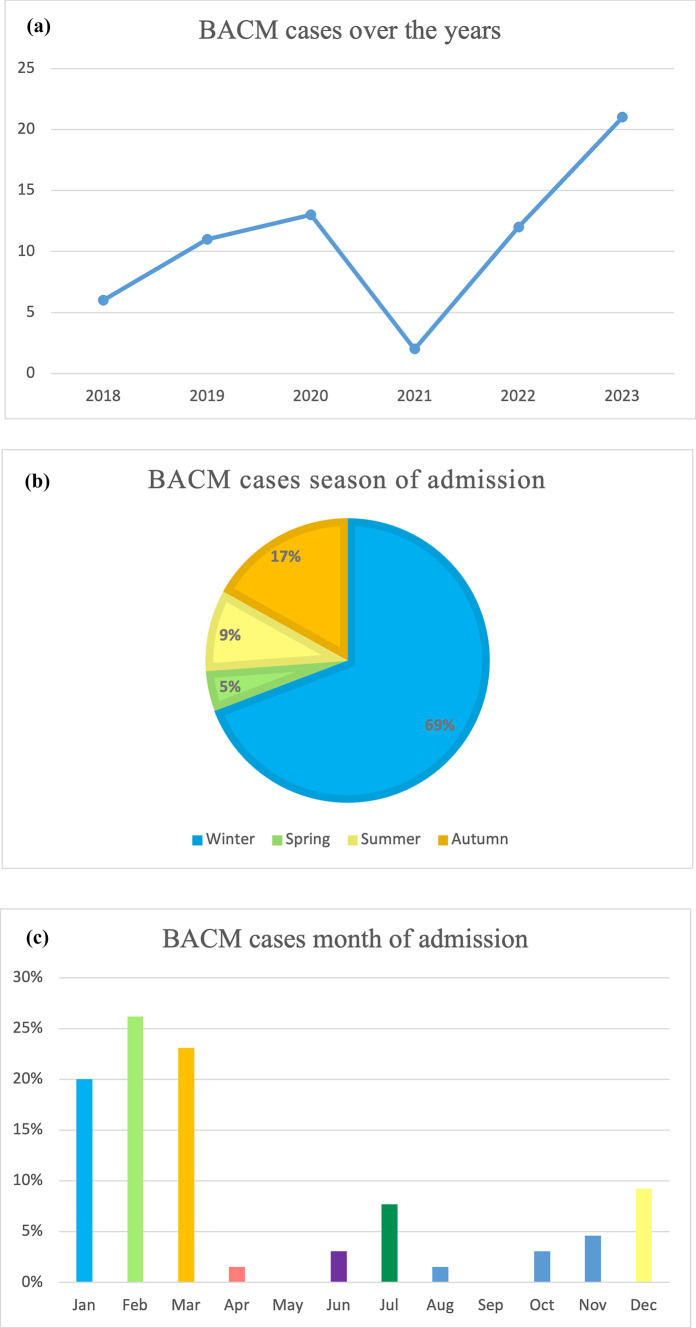
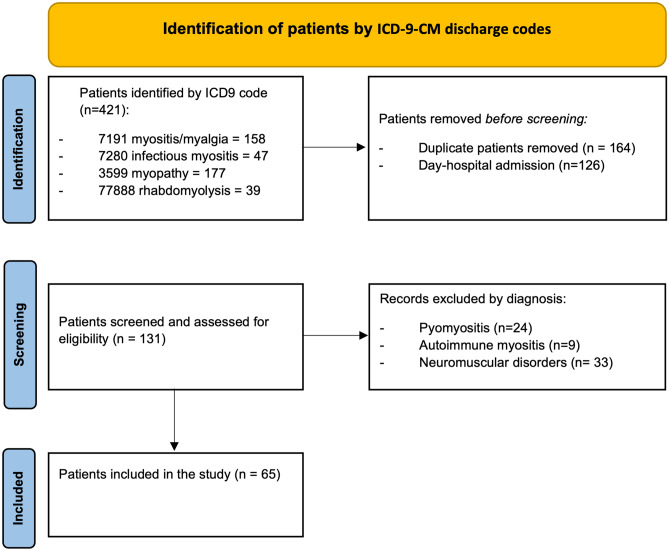
Benign acute childhood myositis (BACM) is a self-limited childhood illness, and viral infections mainly cause it. Clinical and laboratory alterations usually normalize rapidly; generally, the only medical intervention required is supportive (hydration and analgesic medication). The low awareness about BACM often led to delayed diagnosis and unneeded ancillary investigations. This study aims to better characterize the clinical and laboratory features of BACM to improve the diagnostic process and inpatient and outpatient management. We conducted a retrospective study selecting all children admitted to Meyer's Children's Hospital-IRCCS (Florence, Italy) with a diagnosis of BACM over the last 5 years, both those visited at Emergency Department (ED) and those admitted to the Pediatric Unit. Clinical, laboratory, and instrumental data were collected from electronic clinical records and analyzed. Overall, sixty-five patients were enrolled; 49 children were visited and discharged directly from ED, whereas 16 were admitted in the Pediatric or Neurologic Wards. The median age was 6.56 years (IQR 4.9-9.1). Male gender (66.1%) and Caucasian ethnicity (70%) were prevalent. Most patients were admitted during winter, and a second peak was found in autumn. All patients had bilateral calf pain, most of them (87.7%) associated with asthenia and refuse to walk (93.8%). Prodromal symptoms were fever (75.3%), cough (32.3%), coryza (26.1%), sore throat (26.1%), and vomiting (15.3%). The median value of CPK was 1827 U/L (IQR 915.5-2462) at peak. CPK median time to normalization was 7 days (IQR 7-8.5) from the nadir. Influenza B was the virus most frequently BACM associated, followed by Influenza A; a novel association with Sars-CoV-2 has been detected. Two patients had pathogenic variants at the Next Generation Sequencing myopathies panel. Conclusion: School-aged children admitted to the hospital with walking difficulty and myalgia, generally after an upper respiratory tract infection with a moderate CPK elevation, should remind at first of BACM. Rapid complaint resolution and biochemical markers normalization will prevent unnecessary tests and inappropriate therapies. What is Known: • BACM is a self-limited syndrome associated with acute infections. Influenza A and B viruses are the main etiological agents, but BACM may be related to many other microorganisms like Parainfluenza virus, Epstein-Barr virus, Cytomegalovirus, Human herpesvirus 6, Respiratory syncytial virus, Coxsackieviruses, Mycoplasma pneumoniae, Streptococcus pyogenes, Legionella, and Salmonella spp. • Clinical and laboratory alterations usually normalize rapidly; generally, the only medical intervention required is supportive (hydration, analgesic medication). Evolution in rhabdomyolysis and kidney damage is possible but rarely reported. What is New: • Sars-CoV-2 could be an emerging possible cause of BACM. During and after the Sars-CoV-2 outbreak, virus infection seasonality has changed, and so has BACM seasonality. • Screening tests for muscular and metabolic disorders are recommended in recurrent myositis and/or cases with marked CPK elevation (≥ 5000 U/L).
良性急性儿童肌炎(BACM)是一种自限性儿童疾病,主要由病毒感染引起。临床和实验室改变通常迅速恢复正常;一般来说,唯一需要的医疗干预是支持性治疗(补液和止痛药物)。对 BACM 的认识不足常常导致诊断延迟和不必要的辅助检查。本研究旨在更好地描述 BACM 的临床和实验室特征,以改善诊断过程和住院和门诊管理。我们进行了一项回顾性研究,选择了过去 5 年来在迈耶儿童医院-IRCCS(意大利佛罗伦萨)因 BACM 住院的所有儿童,包括在急诊科就诊和住院到儿科或神经科病房的儿童。从电子病历中收集了临床、实验室和仪器数据,并进行了分析。共有 65 名患者入组;49 名儿童在急诊科就诊并直接出院,16 名在儿科或神经科病房住院。中位年龄为 6.56 岁(IQR 4.9-9.1)。男性(66.1%)和白种人(70%)居多。大多数患者在冬季入院,秋季出现第二个高峰。所有患者均有双侧小腿疼痛,其中 87.7%(93.8%)伴有乏力和拒绝行走。前驱症状为发热(75.3%)、咳嗽(32.3%)、鼻塞(26.1%)、咽痛(26.1%)和呕吐(15.3%)。CPK 峰值时中位数为 1827 U/L(IQR 915.5-2462)。CPK 从最低点恢复正常的中位数时间为 7 天(IQR 7-8.5)。乙型流感是与 BACM 最相关的病毒,其次是甲型流感;还检测到与 SARS-CoV-2 的新关联。两名患者在下一代测序肌病面板中存在致病性变异。结论:学龄儿童因行走困难和肌痛住院,一般在上呼吸道感染后 CPK 中度升高,首先应考虑 BACM。快速缓解症状和生化标志物恢复正常将预防不必要的检查和不适当的治疗。已知的:• BACM 是一种与急性感染相关的自限性综合征。流感 A 和 B 病毒是主要的病原体,但 BACM 可能与许多其他微生物有关,如副流感病毒、Epstein-Barr 病毒、巨细胞病毒、人类疱疹病毒 6、呼吸道合胞病毒、柯萨奇病毒、肺炎支原体、链球菌、军团菌和沙门氏菌。•临床和实验室改变通常迅速恢复正常;一般来说,唯一需要的医疗干预是支持性治疗(补液、止痛药物)。横纹肌溶解症和肾脏损伤的演变是可能的,但很少有报道。新的发现:• SARS-CoV-2 可能是 BACM 的一个新的可能病因。在 SARS-CoV-2 爆发期间和之后,病毒感染的季节性发生了变化,BACM 的季节性也发生了变化。•对于反复发作的肌炎和/或 CPK 明显升高(≥5000 U/L)的患者,建议进行肌肉和代谢疾病的筛查试验。