Mehta Milap, Reynolds Maegan, Yee Jennifer
The Ohio State University, Department of Emergency Medicine, Columbus OH.
J Educ Teach Emerg Med. 2020 Apr 15;5(2):S26-S54. doi: 10.21980/J80S75. eCollection 2020 Apr.
This scenario was developed to educate emergency medicine residents on the diagnosis and management of primary measles encephalitis.
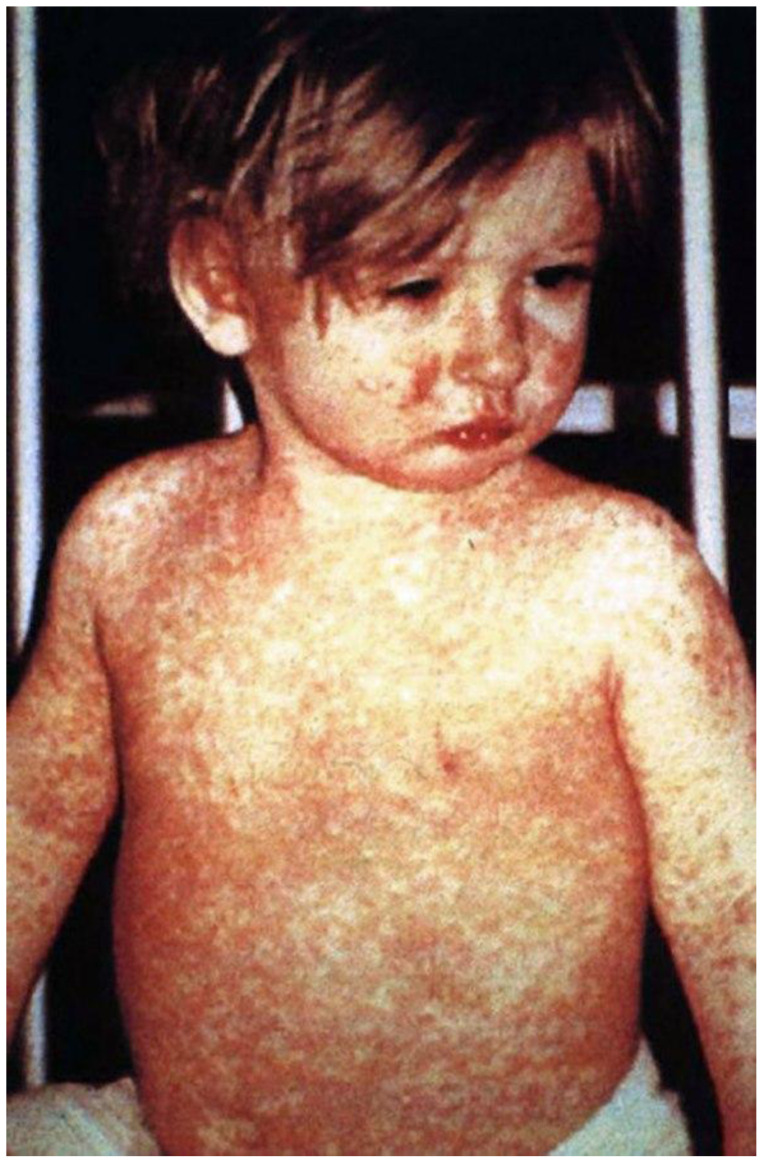
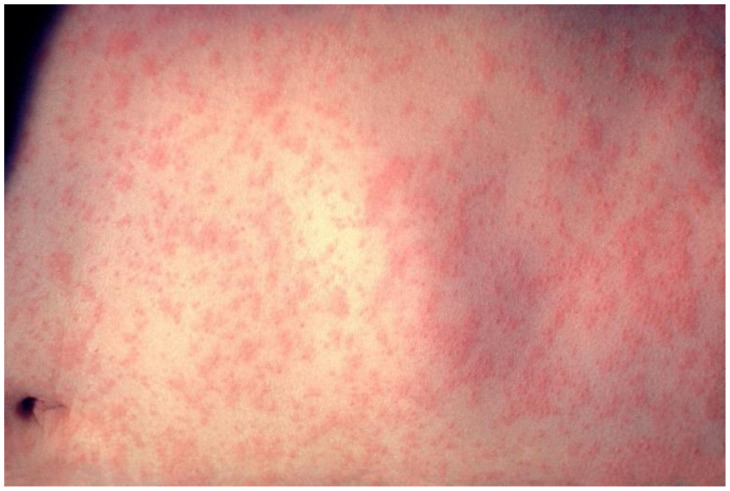
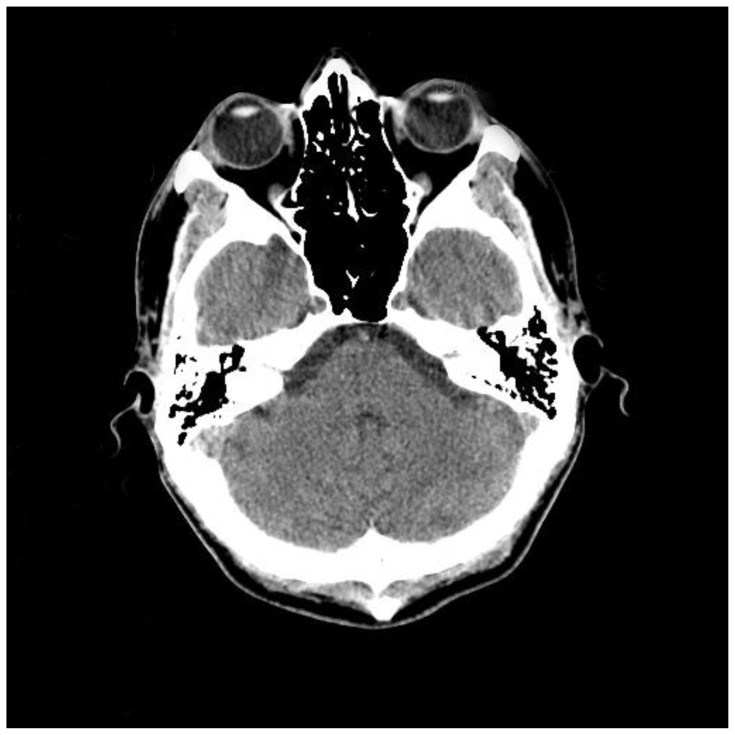
Measles is a highly infectious ribonucleic acid (RNA) virus whose prevalence in the United States has continued to increase despite being declared eliminated in 2000,1 and larger outbreaks have been noted among those who elect not to vaccinate.2 The recommended live-attenuated measles, mumps, and rubella (MMR) vaccine schedule for pediatrics includes one routine dose at 12-15 months of age and a second dose between 4-6 years of age with at least 28 days in between dose administration.1-2 Measles-associated complications include otitis media, pneumonia, laryngotracheobronchitis, diarrhea, and corneal ulceration.2 Patients may also develop central nervous system complications, including primary measles encephalitis, acute post-infectious measles encephalomyelitis, measles inclusion body encephalitis, and subacute sclerosing panencephalitis. Primary measles encephalitis and measles inclusion body encephalitis involve an active ongoing measles infection.3 We will focus on primary measles encephalitis for this case scenario. One out of every 1000 measles patients will develop primary measles encephalitis,1 with onset typically occurring within seven days of the measles prodrome. Treatment is largely supportive. Mortality from primary measles encephalitis is 10%-15%, with an additional 25% developing permanent neurodevelopmental sequalae.3 It is critical to maintain a high index of suspicion for this diagnosis, to place the patient in airborne precautions to protect other immunocompromised individuals, and to transfer to a pediatric intensive care unit (PICU).
At the conclusion of the simulation session, learners will be able to: 1) Obtain a relevant focused history, including immunization status, associated symptoms, sick contacts, and travel history. 2) Develop a differential for fever, rash, and altered mental status in a pediatric patient. 3) Discuss management of primary measles encephalitis, including empiric broad spectrum antibiotics and antiviral treatment. 4) Discuss appropriate disposition of the patient from pediatric emergency departments, community hospitals, and freestanding emergency departments, including appropriate time to call for transfer and the appropriate time to transfer this patient during emergency department (ED) workup. 5) Review types of isolation and indications for each.
This session was conducted using high-fidelity simulation, followed by a debriefing session and lecture on the diagnosis, differential diagnosis, and management of primary measles encephalitis. Debriefing methods may be left to the discretion of participants, but the authors have utilized advocacy-inquiry techniques. This scenario may also be run as an oral board case.
Our residents are provided a survey at the completion of the debriefing session so they may rate different aspects of the simulation, as well as provide qualitative feedback on the scenario.
Feedback from the residents was overwhelmingly positive with an average score of 7 (consistently effective/very good or extremely effective/outstanding) across all categories. The subsequent debriefings allowed for multiple areas of discussion, including differential diagnoses of fever and rash, the clinical presentation of measles, empiric treatment of meningitis/encephalitis, types and indications of isolation, when to call for transfer to a pediatric center, and when a child is deemed stable enough for transfer.
This is a cost-effective method for reviewing primary measles encephalitis. There are multiple measles complications that may be reviewed via simulation, including pneumonia and dehydration from diarrhea. We encourage readers to utilize clinical photos of measles rashes, because this was difficult to capture via standard moulage techniques.
Medical simulation, measles, primary measles encephalitis, encephalitis, infectious disease, emergency medicine, pediatric emergency medicine.
设计此病例是为了培训急诊医学住院医师对原发性麻疹脑炎的诊断和管理。
麻疹是一种高度传染性的核糖核酸(RNA)病毒,尽管美国在2000年宣布已消除麻疹,但它的流行率仍在持续上升,并且在那些选择不接种疫苗的人群中出现了更大规模的疫情。儿科推荐的减毒活麻疹、腮腺炎和风疹(MMR)疫苗接种计划包括在12至15个月龄时接种一剂常规疫苗,以及在4至6岁之间接种第二剂,两剂接种之间至少间隔28天。麻疹相关并发症包括中耳炎、肺炎、喉气管支气管炎、腹泻和角膜溃疡。患者还可能出现中枢神经系统并发症,包括原发性麻疹脑炎、急性感染后麻疹脑脊髓炎、麻疹包涵体脑炎和亚急性硬化性全脑炎。原发性麻疹脑炎和麻疹包涵体脑炎涉及正在进行的活动性麻疹感染。本病例将重点关注原发性麻疹脑炎。每1000例麻疹患者中就有1例将发展为原发性麻疹脑炎,通常在麻疹前驱症状出现后的七天内发病。治疗主要是支持性的。原发性麻疹脑炎的死亡率为10% - 15%,另有25%的患者会出现永久性神经发育后遗症。对此诊断保持高度怀疑指数、对患者采取空气传播预防措施以保护其他免疫功能低下的个体,并将患者转至儿科重症监护病房(PICU)至关重要。
在模拟课程结束时,学习者将能够:1)获取相关的重点病史,包括免疫接种状况、相关症状、患病接触者和旅行史。2)对儿科患者的发热、皮疹和精神状态改变进行鉴别诊断。3)讨论原发性麻疹脑炎的管理,包括经验性广谱抗生素和抗病毒治疗。4)讨论儿科急诊科、社区医院和独立急诊科对患者的适当处置,包括呼叫转诊的适当时间以及在急诊科检查期间将该患者转诊的适当时间。5)回顾隔离类型及其适应证。
本课程采用高保真模拟进行,随后进行总结汇报和关于原发性麻疹脑炎的诊断、鉴别诊断及管理的讲座。总结汇报方法可由参与者自行决定,但作者采用了倡导性询问技巧。此病例也可作为口试病例进行。
在总结汇报课程结束时,我们为住院医师提供了一份调查问卷,以便他们对模拟的不同方面进行评分,并对病例提供定性反馈。
住院医师的反馈总体积极,所有类别平均得分为7分(始终有效/非常好或极其有效/出色)。随后的总结汇报允许进行多个领域的讨论,包括发热和皮疹的鉴别诊断、麻疹的临床表现、脑膜炎/脑炎的经验性治疗、隔离类型和适应证、何时呼叫转诊至儿科中心以及何时儿童被认为足够稳定可以转诊。
这是一种复习原发性麻疹脑炎的经济有效的方法。通过模拟可以复习多种麻疹并发症,包括肺炎和腹泻引起的脱水。我们鼓励读者使用麻疹皮疹的临床照片,因为通过标准的人体模型技术很难捕捉到。
医学模拟、麻疹、原发性麻疹脑炎、脑炎、传染病、急诊医学、儿科急诊医学