Keller Chad R, Nebor Ivanna, Choi David, Moreno Kattia, Patil Yash J
University of Cincinnati College of Medicine, Department of Otolaryngology Head and Neck Surgery, Cincinnati, OH.
J Educ Teach Emerg Med. 2022 Apr 15;7(2):I1-I9. doi: 10.21980/J85M0B. eCollection 2022 Apr.
Our reusable low-cost peritonsillar abscess simulator (PTA) simulator is designed to train emergency medicine (EM) residents, fellows, and medical students. Trainees who are interested in otolaryngology (OTL) or this specific disease may also benefit from this simulator.
Peritonsillar abscess is one of the most common deep infections 1 of the head and neck, accounting for 7589 consultations and 11069 hospital bed days in the UK between 2009-2010.1,2 Emergency medicine physicians commonly treat this pathology with surgical and medical modalities. Not only is this a common diagnosis, but there is a significant cost associated with the evaluation and management of primary PTA. 3Demands for high-volume patient care and good patient outcomes are increasing in a medical climate of limited financial resources and resident work hours. Given these complexities, medical education is viewing simulation training, with proven success in various surgical specialties, as a valuable addition to resident education and patient safety. 3-5The PTA is the collection of pus in the space between the palatine tonsil and its capsule. Successfully locating the abscess is crucial because it prevents the unwanted damage of nearby vascular structures, patient discomfort, and failure to treat the infection. Management of peritonsillar abscess is primarily surgical and includes incision and drainage (I & D), needle aspiration, or Quinsy tonsillectomy.The simulator provides a realistic characteristic of typical PTA presentations, such as uvula deviation, swelling, trismus, and purulence during aspiration. While learning to drain a PTA, trainees must locate the infection with a needle without injury to the surrounding structures of the oral cavity and deep structures of the neck. The discomfort caused during this procedure can be unsettling for both physician and patient. Simulation use and testing enable the trainee to develop familiarity with handling instruments, increase comfort with the sequence of a procedure, and improve confidence in the ability to perform a procedure safely.6,7,8 Simulators provide improved patient outcomes and increased EM residents' comfort level.
By the end of this training session, learners will be able to: 1) locate the abscess, 2) perform needle aspiration, and 3) develop dexterity in maneuvering instruments in the small three-dimensional confines of the oral cavity without causing injury to local structures.
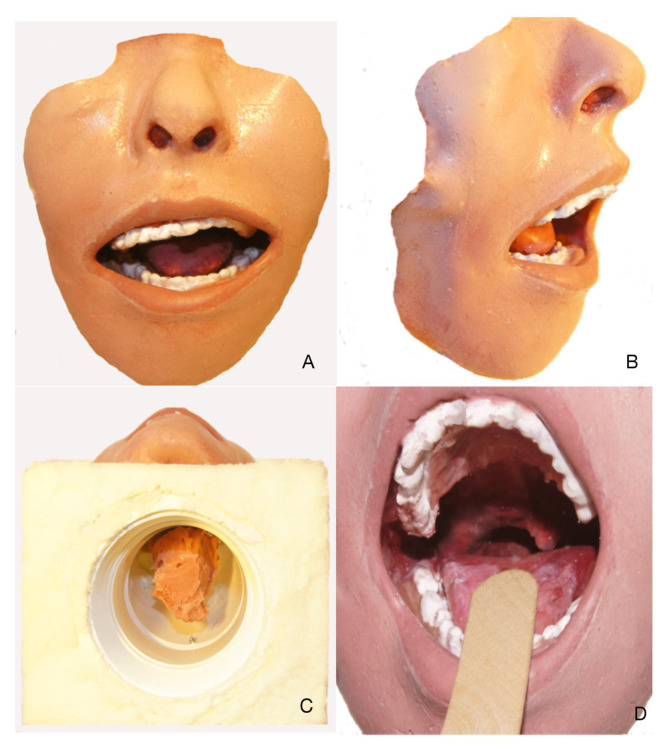
Our PTA simulator was fabricated with a low-cost, non-degradable material and is the first known PTA simulator that used a validated survey for fidelity assessment. The simulator was fabricated using a silicone mold to mimic the oral cavity and oropharynx. A simulated abscess pocket consisting of saline encased in balloon material was placed in the proper anatomic location, allowing for abscess simulation on either side of the oropharynx model. The time to fabricate the model averaged 20 hours. The simulator was manufactured with low-cost materials at an expense of 45 USD and could be easily reproduced by any EM residency program.
Twenty-one participants were instructed to expose and drain the simulated abscess. The model was evaluated using The Michigan Standard Simulation Experience Scale (MiSSES).7 Participants scored the simulator in five categories: Self-efficacy, fidelity, educational value, teaching quality, and the overall rating on a 5-point Likert scale of simulator. Overall rating and global evaluation scores were compared by groups (Group 1, Group 2) between training level (residents and attendings), specialty (emergency and otolaryngology), and previous experience (<5 or ≥5 drainages).Convenience sampling was used to determinate the sample. Variables were summarized using the mean and standard deviation for continuous variables and percentages and frequencies for categorical variables. The MiSSES was scored as previously described in the literature.7 The Kolmogorov-Smirnov test was used to test for normal distribution of the variables. T-test for independent samples was performed to determinate if there exists a difference between groups in perception of a PTA simulator. The statistical analyses were performed using SPSS version 20.0 Armonk, NY: IBM.
Twenty-one participants were enrolled in the study: residents (n=15) and attending (n=6) from OTL and EM departments. The simulator's plasticity allowed multiple attempts of needle aspiration and drainage without degradation and received high ratings on teaching quality, fidelity, and educational value. This PTA simulator achieved high fidelity ratings in the standard simulator's assessment survey for realism of environment, simulation of trismus, uvular deviation, and realism of the mucosal surfaces. On the MiSSES, the model received positive ratings (range 3.6 to 4.9). The highest rating was on teaching quality (4.9), fidelity (4.6), and educational value (4.5) (Table 1). We found that self-efficacy and teaching quality sections were rated higher for those who had less experience (≥5 PTA drainage), while fidelity was rated higher for OTL. The overall rating average was 4 and was higher of attendings, OTL, and those with less experience. All comparisons between groups were not statically significant (Table 2). About 76% of participants found that the simulator can be used in training with slight improvement or no improvement needed. (Table 3).
With favorable participant ratings and comments, we believe that this tool can offer high-fidelity simulation at a low cost. Widespread use may be possible, allowing training of EM residents in performing instrumentation of PTA in a controlled simulation environment. We have created a reusable low-cost PTA simulator that achieved a high score fidelity in a standard simulator's assessment survey.
Peritonsillar abscess, oropharynx, emergency medicine residency, otolaryngology residency training.
我们的可重复使用的低成本扁桃体周围脓肿模拟器(PTA)旨在培训急诊医学(EM)住院医师、研究员和医学生。对耳鼻喉科(OTL)或这种特定疾病感兴趣的受训人员也可能从该模拟器中受益。
扁桃体周围脓肿是头颈部最常见的深部感染之一,在2009 - 2010年间,英国有7589例会诊和11069个住院日。1,2急诊医学医生通常采用手术和药物治疗这种病症。这不仅是一种常见诊断,而且原发性PTA的评估和管理成本高昂。3在财政资源有限和住院医师工作时间受限的医疗环境中,对大量患者护理和良好患者预后的需求日益增加。鉴于这些复杂性,医学教育将在各种外科专业已证明成功的模拟培训视为住院医师教育和患者安全的宝贵补充。3 - 5PTA是腭扁桃体与其包膜之间间隙中的脓液积聚。成功定位脓肿至关重要,因为它可防止对附近血管结构造成不必要的损伤、患者不适以及治疗感染失败。扁桃体周围脓肿的管理主要是手术治疗,包括切开引流(I&D)、针吸或扁桃体切除术。该模拟器具有典型PTA表现的逼真特征,如悬雍垂偏斜、肿胀、牙关紧闭以及抽吸时的化脓。在学习引流PTA时,受训人员必须用针定位感染部位,同时避免损伤口腔周围结构和颈部深部结构。此过程中引起的不适对医生和患者来说都可能令人不安。模拟使用和测试能使受训人员熟悉器械操作,增加对手术流程的舒适度,并提高安全执行手术的信心。6,
7,8模拟器可改善患者预后并提高急诊医学住院医师的舒适度。
在本次培训课程结束时,学习者将能够:1)定位脓肿,2)进行针吸,3)在口腔的小三维空间内灵活操作器械而不损伤局部结构。
我们的PTA模拟器采用低成本、不可降解材料制造,是首个使用经过验证的调查进行逼真度评估的已知PTA模拟器。该模拟器使用硅胶模具制作以模拟口腔和口咽。一个由包裹在气球材料中的盐水组成的模拟脓肿腔放置在适当的解剖位置,可在口咽模型的两侧进行脓肿模拟。制作模型的平均时间为20小时。该模拟器采用低成本材料制造,成本为45美元,任何急诊医学住院医师培训项目都可轻松复制。
21名参与者被指导暴露并引流模拟脓肿。使用密歇根标准模拟体验量表(MiSSES)对模型进行评估。7参与者在五个类别中对模拟器进行评分:自我效能感、逼真度、教育价值、教学质量以及模拟器的总体评分,采用5点李克特量表。通过组(第1组、第2组)比较总体评分和综合评估分数,比较培训水平(住院医师和主治医师)、专业(急诊和耳鼻喉科)以及既往经验(<5次或≥5次引流)。采用便利抽样确定样本。连续变量使用均值和标准差进行汇总,分类变量使用百分比和频率进行汇总。MiSSES的评分如文献中先前所述。7使用柯尔莫哥洛夫 - 斯米尔诺夫检验来检验变量的正态分布。进行独立样本t检验以确定不同组在对PTA模拟器的认知上是否存在差异。使用SPSS 20.0版(纽约州阿蒙克:IBM公司)进行统计分析。
21名参与者纳入研究:来自耳鼻喉科和急诊医学科的住院医师(n = 15)和主治医师(n = 6)。模拟器的可塑性允许多次进行针吸和引流尝试而不降解,在教学质量、逼真度和教育价值方面获得高分。该PTA模拟器在标准模拟器评估调查中,在环境逼真度、牙关紧闭模拟、悬雍垂偏斜以及黏膜表面逼真度方面获得高逼真度评分。在MiSSES上,该模型获得了积极评分(范围为3.6至4.9)。最高评分在教学质量(4.9)、逼真度(4.6)和教育价值(4.5)方面(表1)。我们发现,自我效能感和教学质量部分对于经验较少(≥5次PTA引流)的人评分较高,而逼真度对于耳鼻喉科评分较高。总体评分平均为4分,主治医师、耳鼻喉科医生以及经验较少的人评分更高。组间所有比较均无统计学意义(表2)。约76%的参与者发现该模拟器可用于培训,只需稍作改进或无需改进。(表3)
鉴于参与者的良好评分和评论,我们认为该工具能够以低成本提供高逼真度模拟。可能会得到广泛应用,从而能够在可控的模拟环境中培训急诊医学住院医师进行PTA的器械操作。我们创建了一种可重复使用的低成本PTA模拟器,在标准模拟器评估调查中获得了高逼真度评分。
扁桃体周围脓肿、口咽、急诊医学住院医师培训、耳鼻喉科住院医师培训