Department of Critical Care Medicine, Yokohama City University Hospital, 3-9 Fukuura, Kanazawa-ku, Yokohama, Kanagawa, 236-0004, Japan.
Department of Emergency and Critical Care Medicine, Hitachi General Hospital, 2-1-1, Jonan-cho, Hitachi, Ibaraki, 317-0077, Japan.
Crit Care. 2023 Jul 21;27(1):294. doi: 10.1186/s13054-023-04583-7.
Vasopressin is a second-line vasoactive agent for refractory septic shock. Vasopressin loading is not generally performed because of the lack of evidence for its effects and safety. However, based on our previous findings, we hypothesized it can predict the responsibility to vasopressin infusion with safety, and prospectively examined it in the present study.
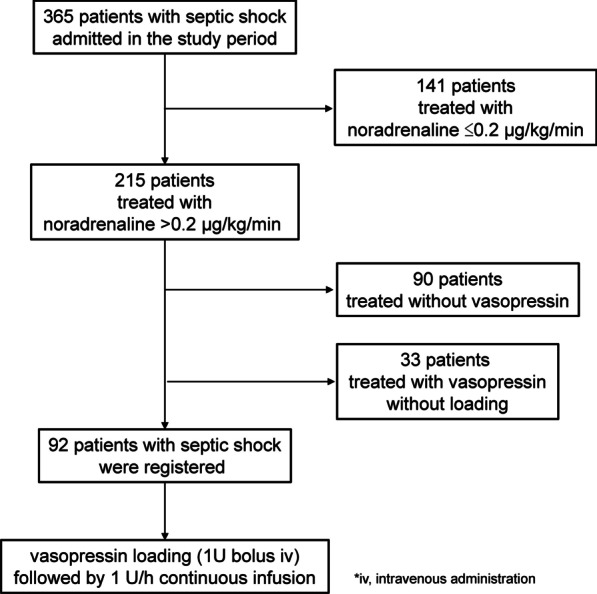
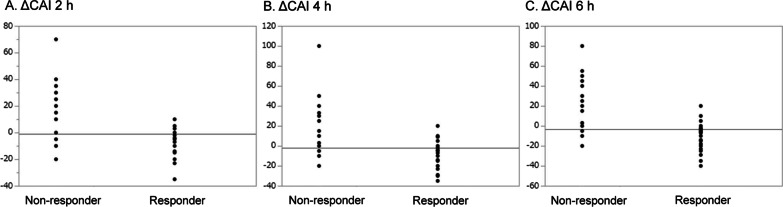
Vasopressin loading was performed via the intravenous administration of a bolus of 1 U, followed by its continuous infusion at 1U/h in patients with septic shock treated with ≥ 0.2 μg/kg/min noradrenaline. An arterial pressure wave analysis was conducted, and endocrinological tests were performed immediately prior to vasopressin loading. We classified patients into responders/non-responders based on mean arterial pressure (MAP) changes after vasopressin loading. Based on our previous findings, the lower tertile of MAP changes was selected as the cut-off. The change in the catecholamine index (CAI) after 6 h was assigned as the primary outcome. Digital ischemia, mesenteric ischemia, and myocardial ischemia during the admission period were prospectively and systematically recorded as adverse events.
Ninety-two patients were registered during the study period and examined. Sixty-two patients with a MAP change > 22 mmHg were assigned as responders and the others as non-responders. Blood adrenocorticotropic hormone levels were significantly higher in non-responders. Stroke volume variations were higher in responders before loading, while stroke volume and dP/dt were higher in responders after loading. Median CAI changes were - 10 in responders and 0 in non-responders, which was significantly lower in the former (p < 0.0001). AUROC of MAP change with vasopressin loading to predict CAI change < 0 after continuous infusion was 0.843 with sensitivity of 0.92 and specificity of 0.77. Ischemia events were observed in 5 cases (5.4%).
Vasopressin loading may be safely introduced for septic shock. Vasopressin loading may be used to predict responses to its continuous infusion and select appropriate strategies to increase blood pressure.
加压素是治疗难治性感染性休克的二线血管活性药物。由于缺乏其疗效和安全性的证据,通常不进行加压素负荷。然而,基于我们之前的发现,我们假设它可以安全地预测对加压素输注的反应,并在本研究中前瞻性地进行了检查。
在接受≥0.2μg/kg/min去甲肾上腺素治疗的感染性休克患者中,通过静脉注射 1U 负荷量,随后以 1U/h 的速度持续输注加压素。进行动脉压力波分析,并在加压素负荷前进行内分泌测试。我们根据加压素负荷后平均动脉压(MAP)的变化将患者分为反应者/无反应者。基于我们之前的发现,选择 MAP 变化的较低三分位数作为截止值。6 小时后儿茶酚胺指数(CAI)的变化被指定为主要结局。在入院期间,前瞻性和系统地记录数字缺血、肠系膜缺血和心肌缺血作为不良事件。
在研究期间共登记了 92 例患者并进行了检查。62 例 MAP 变化>22mmHg 的患者被分配为反应者,其余为无反应者。无反应者的促肾上腺皮质激素水平明显较高。负荷前反应者的每搏量变异较高,而负荷后反应者的每搏量和 dP/dt 较高。反应者的中位数 CAI 变化为-10,无反应者为 0,前者明显较低(p<0.0001)。MAP 变化与加压素负荷后连续输注预测 CAI 变化<0 的 AUROC 为 0.843,敏感性为 0.92,特异性为 0.77。5 例(5.4%)出现缺血事件。
加压素负荷可安全用于感染性休克。加压素负荷可用于预测对其连续输注的反应,并选择适当的策略来升高血压。