Salton Francesco, Confalonieri Paola, Meduri Gianfranco Umberto, Mondini Lucrezia, Trotta Liliana, Barbieri Mariangela, Bozzi Chiara, Torregiani Chiara, Lerda Selene, Bellan Mattia, Confalonieri Marco, Ruaro Barbara, Tavano Stefano, Pozzan Riccardo
Pulmonology Unit, Department of Medical Surgical and Health Sciences, University Hospital of Cattinara, University of Trieste, 34149 Trieste, Italy.
Department of Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, University of Tennessee Health Science Center, Memphis, TN 38163, USA.
Pharmaceuticals (Basel). 2023 Jun 25;16(7):924. doi: 10.3390/ph16070924.
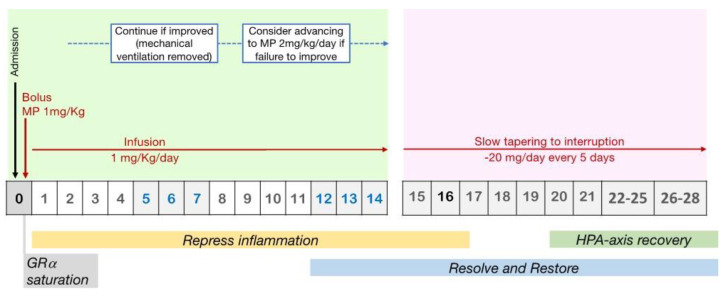
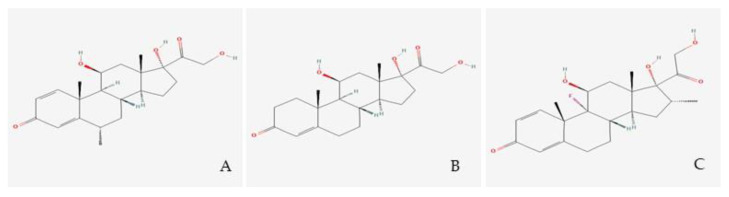
Prolonged, low-dose glucocorticoids (GCs) have shown the highest efficacy among pharmacological and non-pharmacological treatments for COVID-19. Despite the World Health Organization's recommendation against their use at the beginning of the pandemic, GCs at a dose equivalent to dexamethasone 6 mg/day for 10 days are now indicated in all COVID-19 cases who require respiratory support. However, the efficacy of the intervention depends on the timing of initiation, the dose, and other individual factors. Indeed, patients treated with similar GC protocols often experience different outcomes, which do not always correlate with the presence of comorbidities or with the severity of respiratory involvement at baseline. This prompted us to critically review the literature on the rationale, pharmacological principles, and clinical evidence that should guide GC treatment. Based on these data, the best treatment protocol probably involves an initial bolus dose to saturate the glucocorticoid receptors, followed by a continuous infusion to maintain constant plasma levels, and eventually a slow tapering to interruption. Methylprednisolone has shown the highest efficacy among different GC molecules, most likely thanks to its higher ability to penetrate the lung. Decreased tissue sensitivity to glucocorticoids is thought to be the main mechanism accounting for the lower response to the treatment in some individuals. We do not have a readily available test to identify GC resistance; therefore, to address inter-individual variability, future research should aim at investigating clinical, physiological, and laboratory markers to guide a personalized GC treatment approach.
在治疗新型冠状病毒肺炎(COVID-19)的药物和非药物治疗方法中,长期低剂量使用糖皮质激素(GCs)已显示出最高疗效。尽管世界卫生组织在疫情初期建议不要使用糖皮质激素,但目前对于所有需要呼吸支持的COVID-19病例,均建议使用相当于地塞米松6毫克/天的剂量,持续使用10天。然而,干预措施的疗效取决于开始使用的时间、剂量和其他个体因素。事实上,接受类似糖皮质激素治疗方案的患者往往会有不同的结果,这些结果并不总是与合并症的存在或基线时呼吸受累的严重程度相关。这促使我们严格审查有关指导糖皮质激素治疗的理论依据、药理学原理和临床证据的文献。基于这些数据,最佳治疗方案可能包括初始推注剂量以饱和糖皮质激素受体,随后持续输注以维持血浆水平恒定,最终缓慢减量至停药。在不同的糖皮质激素分子中,甲泼尼龙已显示出最高疗效,这很可能归功于其更强的肺部穿透能力。组织对糖皮质激素的敏感性降低被认为是一些个体对治疗反应较低的主要机制。我们目前没有现成的检测方法来识别糖皮质激素抵抗;因此,为了解决个体差异问题未来的研究应致力于调查临床、生理和实验室指标,以指导个性化的糖皮质激素治疗方法。