Department of Global Pediatric Medicine, St Jude Children's Research Hospital, Memphis, TN, USA; Warren Alpert Medical School, Brown University, Providence, RI, USA.
Department of Global Pediatric Medicine, St Jude Children's Research Hospital, Memphis, TN, USA.
Lancet Oncol. 2023 Sep;24(9):967-977. doi: 10.1016/S1470-2045(23)00318-2. Epub 2023 Jul 27.
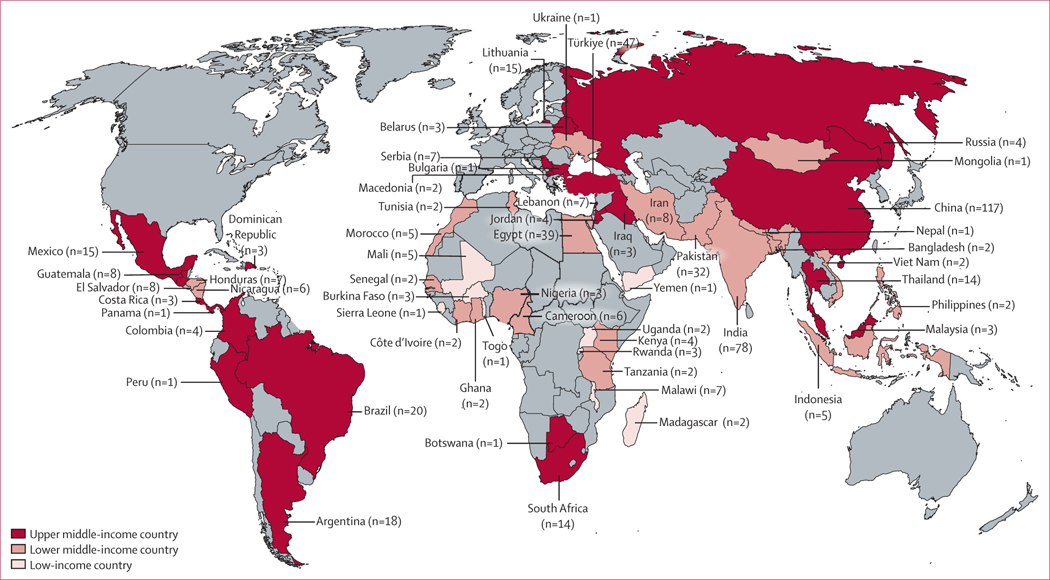
Approximately 90% of children with cancer live in low-income and middle-income countries (LMICs), where 5-year survival is lower than 20%. Treatment-related mortality in high-income countries is approximately 3-5%; however, in LMICs, treatment-related mortality has been reported in up to 45% of children with cancer. This study aimed to systematically explore the burden of treatment-related mortality in children with cancer in LMICs and to explore the association between country income level and treatment-related mortality.
For this systematic review and meta-analysis we identified articles published between Jan 1, 2010, and June 22, 2021, describing treatment-related mortality in paediatric patients (aged 0-21 years) with cancer in LMICs. We searched PubMed, Trip, Web of Science, Embase, and the WHO Global Metric Index databases. The search was limited to full-text articles and excluded case reports (<10 patients) and haematopoietic stem-cell transplantation recipients. Two reviewers independently screened studies for eligibility, extracted data from included publications, and evaluated data quality. Random and mixed-effects models were used to estimate treatment-related mortality burden and trends. The Cochran-Q statistic was used to assess heterogeneity between studies. This study is registered on PROSPERO (CRD42021264849).
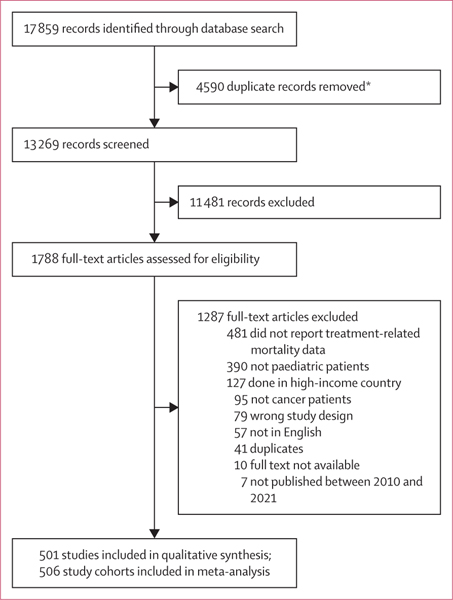
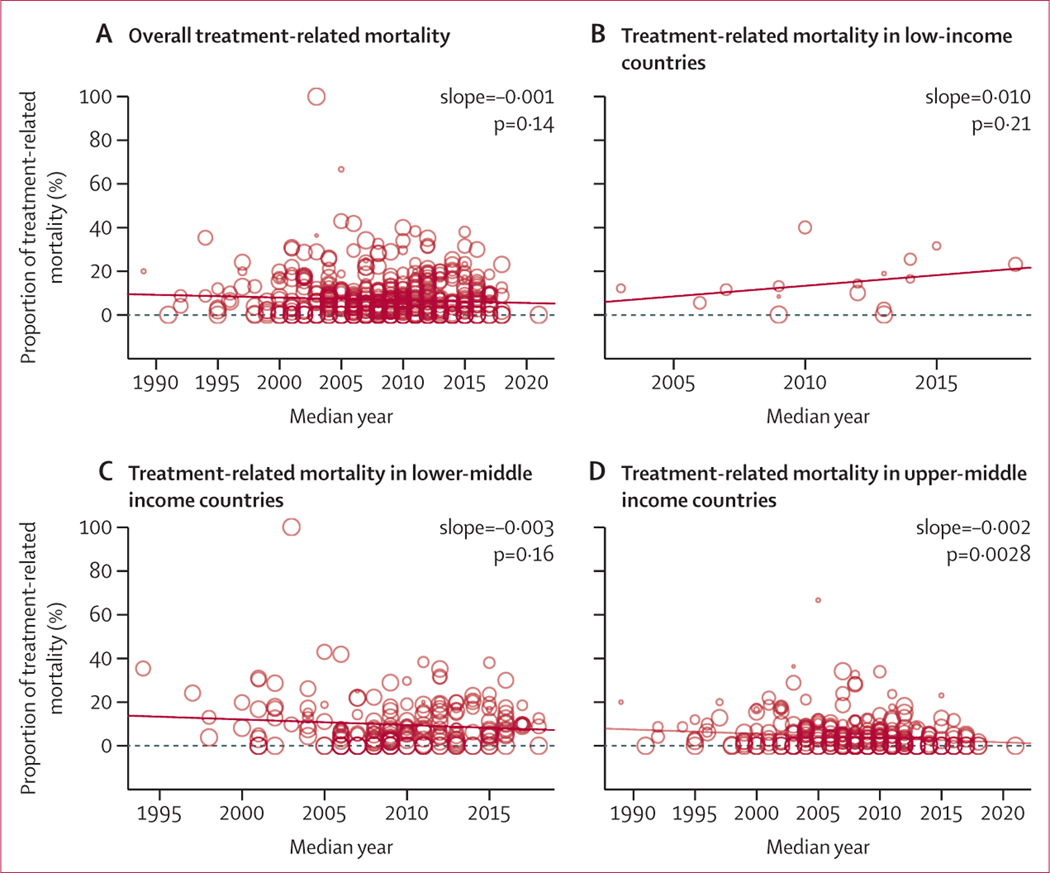
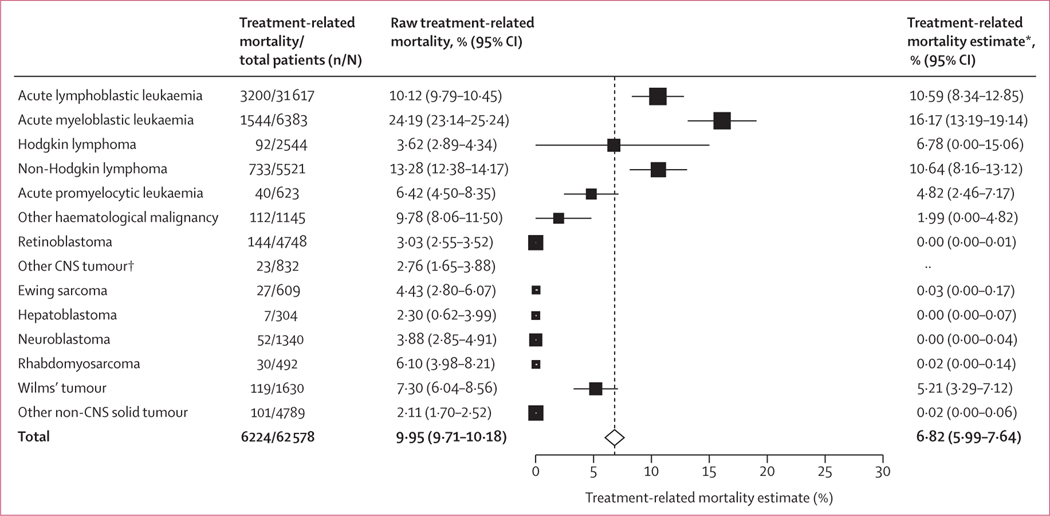
Of 13 269 identified abstracts, 501 studies representing 68 351 paediatric patients with cancer were included. The treatment-related mortality estimate was 6·82% (95% CI 5·99-7·64), accounting for 30·9% of overall mortality (4437 of 14 358 deaths). Treatment-related mortality was inversely related to country income. Treatment-related mortality was 14·19% (95% CI 9·65-18·73) in low-income countries, 9·21% (7·93-10·49) in lower-middle-income countries, and 4·47% (3·42-5·53) in upper-middle-income countries (Cochran-Q 42·39, p<0·0001). In upper-middle-income countries, the incidence of treatment-related mortality decreased over time (slope -0·002, p=0·0028); however, outcomes remained unchanged in low-income (p=0·21) and lower-middle-income countries (p=0·16).
Approximately one in 15 children receiving cancer treatment in LMICs die from treatment-related complications. Although treatment-related mortality has decreased in upper-middle-income countries over time, it remains unchanged in LMICs. There is an urgent need for targeted supportive care interventions to reduce global disparities in childhood cancer survival.
American Lebanese Syrian Associated Charities and National Cancer Institute.
约 90%的癌症患儿生活在低收入和中等收入国家(LMICs),这些国家的 5 年生存率低于 20%。高收入国家的治疗相关死亡率约为 3-5%;然而,在 LMICs,高达 45%的癌症患儿出现了治疗相关的死亡。本研究旨在系统地探讨 LMICs 中癌症患儿的治疗相关死亡率负担,并探讨国家收入水平与治疗相关死亡率之间的关系。
为了进行这项系统评价和荟萃分析,我们在 2010 年 1 月 1 日至 2021 年 6 月 22 日期间,在 Pubmed、Trip、Web of Science、Embase 和世界卫生组织全球度量指数数据库中,检索了描述 LMICs 中儿科癌症患者(年龄 0-21 岁)治疗相关死亡率的文章。我们搜索了全文文章,并排除了病例报告(<10 例)和造血干细胞移植受者。两名评审员独立筛选研究的合格性,从纳入的出版物中提取数据,并评估数据质量。使用随机和混合效应模型来估计治疗相关死亡率负担和趋势。Cochran-Q 统计量用于评估研究之间的异质性。本研究已在 PROSPERO(CRD42021264849)上注册。
在 13269 篇摘要中,有 501 项研究代表了 68351 名患有癌症的儿科患者,纳入了本研究。治疗相关死亡率的估计值为 6.82%(95%CI 5.99-7.64),占总死亡率的 30.9%(4437/14358 例死亡)。治疗相关死亡率与国家收入呈负相关。在低收入国家,治疗相关死亡率为 14.19%(95%CI 9.65-18.73),中下收入国家为 9.21%(7.93-10.49),中上收入国家为 4.47%(3.42-5.53)(Cochran-Q 42.39,p<0.0001)。在上中等收入国家,治疗相关死亡率随时间呈下降趋势(斜率-0.002,p=0.0028);然而,在低收入国家(p=0.21)和中下等收入国家(p=0.16),治疗相关死亡率的结果并没有改变。
在 LMICs 中,大约每 15 名接受癌症治疗的儿童中就有 1 名死于治疗相关并发症。尽管治疗相关死亡率在上中等收入国家随时间推移而下降,但在 LMICs 中并未改变。迫切需要有针对性的支持性护理干预措施,以减少全球儿童癌症生存方面的差异。
美国黎巴嫩叙利亚裔协会慈善基金会和美国国立卫生研究院。