Margato Pazos Júlia, Segnini Tiberti Mariana, Cecilio Hallak Regalo Simone, Nordi Dovigo Lívia, Garcia Patricia Petromilli Nordi Sasso
Department of Social Dentistry, School of Dentistry of Araraquara, Universidade Estadual Paulista, Araraquara, São Paulo, Brazil.
Department of Basic and Oral Biology, School of Dentistry of Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brazil.
PeerJ. 2023 Jul 26;11:e15663. doi: 10.7717/peerj.15663. eCollection 2023.
This study aimed to observe the effect of different finger rest positions on the muscular activity of the hand, forearm, arm, shoulder, thorax, and neck, as well as on the angular deviation from the neutral position of the neck, trunk, upper arm, and forearm on the working side during pre-clinical procedures.
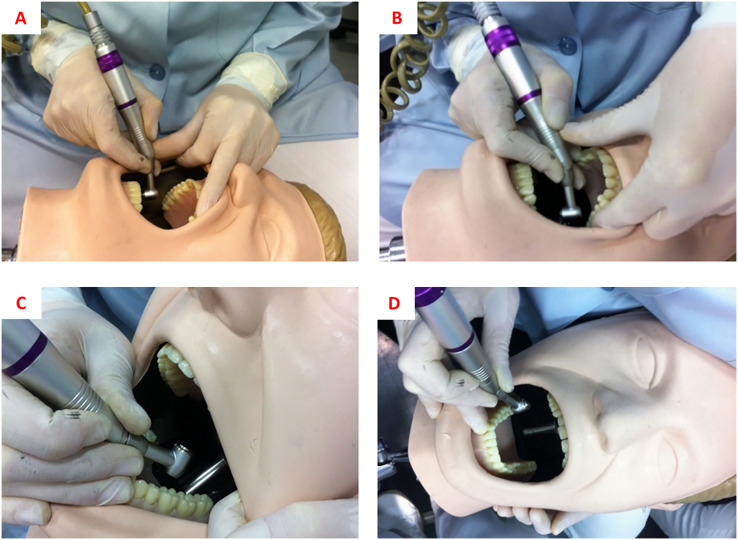
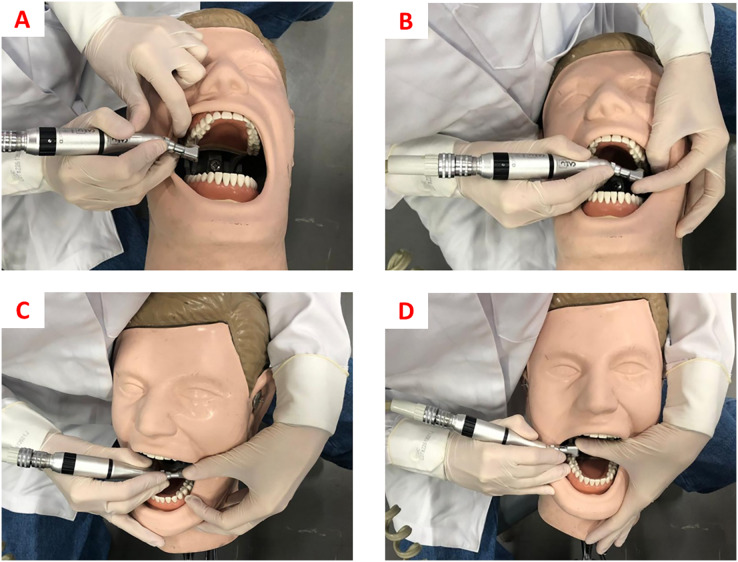
An experimental laboratory study was performed. Response variables were muscle activation of the abductor pollicis, brachioradialis, biceps brachii, deltoid, pectoralis major, and right sternocleidomastoid muscles and angular deviation from the neutral position of the neck, trunk, arm, and forearm during simulated clinical procedures. Independent variable was finger-rest position during cavity preparation (no finger rest, usual rest, and ergonomic rest). Class I cavity preparations (N = 120) were performed on artificial first molars (16, 26, 36, and 46) (N = 120). Muscular activation was assessed by surface electromyography and angular deviations using Software for Postural Assessment (SAPO) version 0.69. One-way analysis of variance and Tukey's or Games-Howell's tests were performed (α = 0.05).
For the sternocleidomastoid muscle, there was no statistically significant difference between the different rest positions. For the deltoid muscle, work with no finger rest resulted in greater muscle activation ( < 0.001) during work on tooth 36. Regarding the pectoralis major and right brachioradialis muscles, we observed that for both teeth 16 and 26, working with ergonomic rest showed less muscle activation. Muscle activation of the right biceps brachii was higher for work with no rest in both the upper and lower arches, differing significantly only from the usual rest in tooth 16 ( < 0.001), usual rest and ergonomic rest in teeth 26 and 46 ( < 0.001), and only ergonomic rest in tooth 36 ( = 0.044). In the right abductor pollicis muscle, work with ergonomic rest resulted in less muscle activation for cavity preparation in teeth 16, 26, and 36, which was significantly different from work with no rest ( = 0.029, < 0.001, and = 0.013, respectively). Regarding angular deviation, it was observed that for tooth 16, there was a greater angular deviation of the arm when performing cavity preparations with no finger rest. For teeth 26 and 46, the ergonomic finger rest provided lower angular deviation from the neutral position of the right arm. For tooth 36, ergonomic rest provided less angular deviation from the neutral neck position.
In general, the use of non-active finger rest during simulated cavity preparations, regardless of the type of rest, provided less muscle activation and angular deviation from the neutral position of the body's upper extremity when performing pre-clinical procedures.
本研究旨在观察不同手指支撑位置对临床前操作过程中手部、前臂、上臂、肩部、胸部和颈部肌肉活动的影响,以及对工作侧颈部、躯干、上臂和前臂偏离中立位角度的影响。
进行了一项实验性实验室研究。反应变量为模拟临床操作过程中拇外展肌、肱桡肌、肱二头肌、三角肌、胸大肌和右侧胸锁乳突肌的肌肉激活情况,以及颈部、躯干、手臂和前臂偏离中立位的角度。自变量为窝洞预备时的手指支撑位置(无手指支撑、常规支撑和符合人体工程学的支撑)。在人工第一磨牙(16、26、36和46)上进行I类窝洞预备(N = 120)。通过表面肌电图评估肌肉激活情况,使用姿势评估软件(SAPO)0.69版测量角度偏差。进行单因素方差分析以及Tukey检验或Games-Howell检验(α = 0.05)。
对于胸锁乳突肌,不同支撑位置之间无统计学显著差异。对于三角肌,在36号牙操作时,无手指支撑的工作导致更大的肌肉激活(< 0.001)。对于胸大肌和右侧肱桡肌,我们观察到在16号牙和26号牙操作时,采用符合人体工程学支撑时肌肉激活较少。在上、下牙弓操作时,右侧肱二头肌在无支撑时的肌肉激活较高,仅在16号牙与常规支撑有显著差异(< 0.001),在26号牙和46号牙与常规支撑和符合人体工程学支撑均有显著差异(< 0.001),在36号牙仅与符合人体工程学支撑有差异(= 0.044)。在右侧拇外展肌,在16号牙、26号牙和36号牙进行窝洞预备时,采用符合人体工程学支撑导致较少的肌肉激活,与无支撑工作有显著差异(分别为= 0.029、< 0.001和= 0.013)。关于角度偏差,观察到在16号牙进行窝洞预备时,无手指支撑时手臂的角度偏差更大。对于26号牙和46号牙,符合人体工程学的手指支撑使右臂偏离中立位的角度更小。对于36号牙,符合人体工程学支撑使颈部偏离中立位的角度更小。
总体而言,在模拟窝洞预备过程中,无论支撑类型如何,使用非主动手指支撑在进行临床前操作时,可减少肌肉激活以及身体上肢偏离中立位的角度偏差。