Ma Ingrid L, Stanley Takara L
Metabolism Unit, Endocrine Division, Massachusetts General Hospital, Boston, MA, USA.
Pediatric Endocrine Division, Massachusetts General Hospital, Boston, MA, USA.
Immunometabolism (Cobham). 2023 Jul 27;5(3):e00030. doi: 10.1097/IN9.0000000000000030. eCollection 2023 Jul.
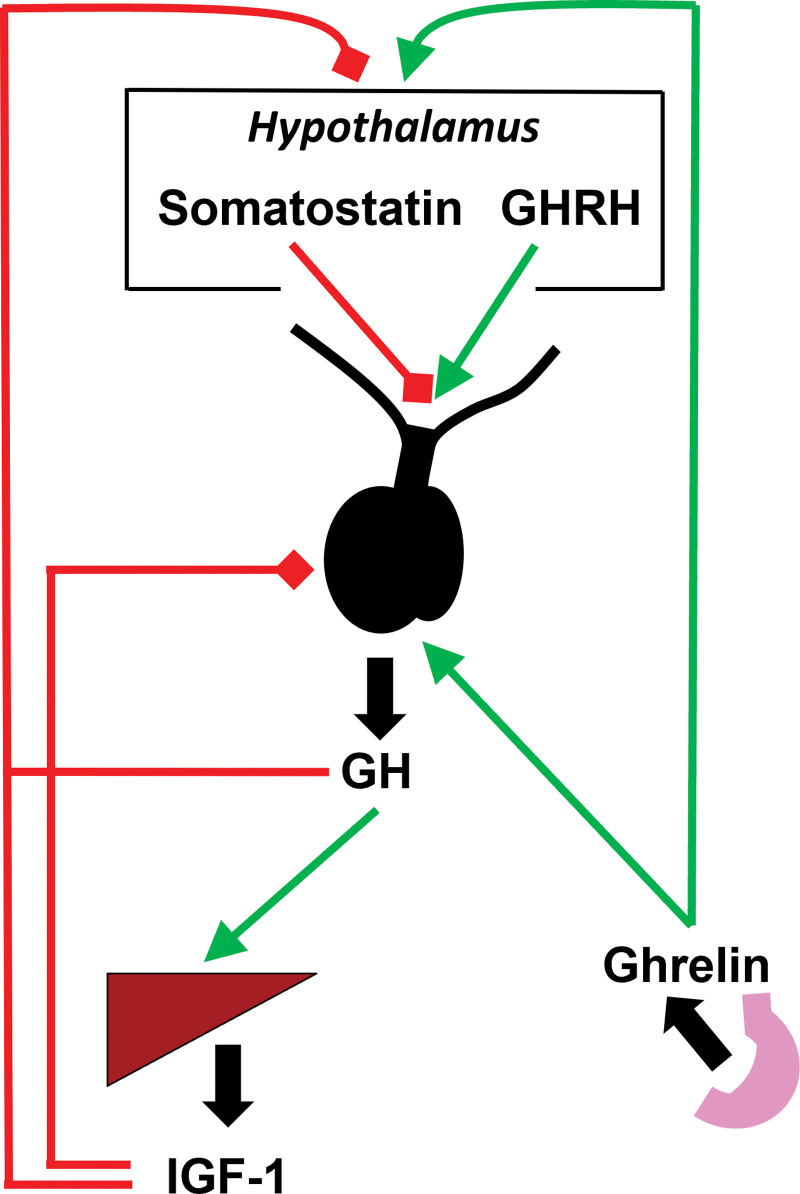
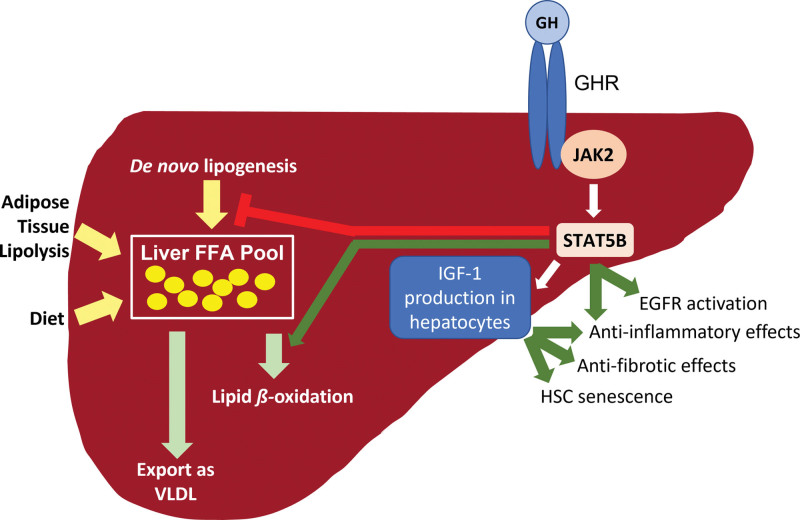
Nonalcoholic fatty liver disease (NAFLD) is a prevalent cause of liver disease and metabolic comorbidities. Obesity is strongly associated with NAFLD and is also a state of relative deficiency of growth hormone (GH). Evidence supports a role of reduced GH and insulin-like growth factor-1 (IGF-1) in NAFLD pathogenesis. Physiological actions of GH in the liver include suppression of de novo lipogenesis (DNL) and promotion of lipid beta-oxidation, and GH also appears to have anti-inflammatory actions. Physiologic actions of IGF-1 include suppression of inflammatory and fibrogenic pathways important in the evolution from steatosis to steatohepatitis and fibrosis. Rodent models of impaired hepatic GH signaling show the development of steatosis, sometimes accompanied by inflammation, hepatocellular damage, and fibrosis, and these changes are ameliorated by treatment with GH and/or IGF-1. In humans, individuals with GH deficiency and GH resistance demonstrate an increased prevalence of NAFLD compared to controls, with improvement in hepatic lipid, steatohepatitis, and fibrosis following GH replacement. As a corollary, individuals with GH excess demonstrate lower hepatic lipid compared to controls along with increased hepatic lipid following treatment to normalize GH levels. Clinical trials demonstrate that augmentation of GH reduces hepatic lipid content in individuals with NAFLD and may also ameliorate steatohepatitis and fibrosis. Taken together, evidence supports an important role for perturbations in the GH/IGF-1 axis as one of the pathogenic mechanisms of NAFLD and suggests that further study is needed to assess whether augmentation of GH and/or IGF-1 may be a safe and effective therapeutic strategy for NAFLD.
非酒精性脂肪性肝病(NAFLD)是肝脏疾病和代谢合并症的常见病因。肥胖与NAFLD密切相关,且也是生长激素(GH)相对缺乏的一种状态。有证据支持GH和胰岛素样生长因子-1(IGF-1)减少在NAFLD发病机制中所起的作用。GH在肝脏中的生理作用包括抑制从头脂肪生成(DNL)和促进脂质β-氧化,并且GH似乎还具有抗炎作用。IGF-1的生理作用包括抑制在从脂肪变性发展为脂肪性肝炎和肝纤维化过程中起重要作用的炎症和纤维化途径。肝脏GH信号受损的啮齿动物模型显示出脂肪变性的发展,有时伴有炎症、肝细胞损伤和纤维化,而用GH和/或IGF-1治疗可改善这些变化。在人类中,与对照组相比,GH缺乏和GH抵抗的个体NAFLD患病率增加,在进行GH替代治疗后,肝脏脂质、脂肪性肝炎和纤维化有所改善。相应地,与对照组相比,GH分泌过多的个体肝脏脂质较低,而在治疗使GH水平正常化后肝脏脂质增加。临床试验表明,增加GH可降低NAFLD患者的肝脏脂质含量,还可能改善脂肪性肝炎和纤维化。综上所述,有证据支持GH/IGF-1轴紊乱作为NAFLD的致病机制之一发挥重要作用,并表明需要进一步研究以评估增加GH和/或IGF-1是否可能是一种安全有效的NAFLD治疗策略。