Sugawara Kazuhiro, Takeuchi Toshiki, Harada Kuniaki, Taki Marina, Fujimura Ikumi, Kogami Yuichi, Furuta Ryoichi
Department of Physical Therapy, School of Health Sciences, Sapporo Medical University, Sapporo, Japan.
Department of Rehabilitation, Kashiwaba Neurosurgical Hospital, Sapporo, Japan.
Front Neurol. 2023 Jul 14;14:1203450. doi: 10.3389/fneur.2023.1203450. eCollection 2023.
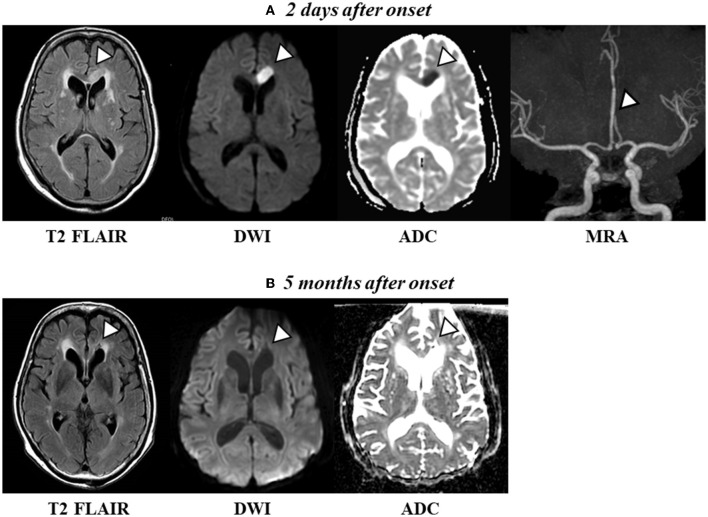
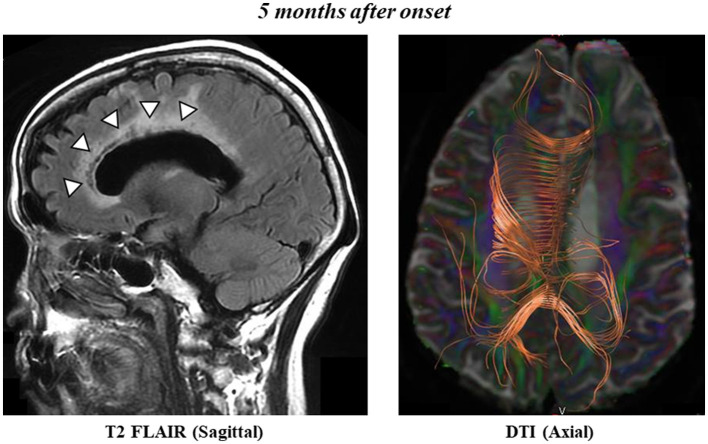
Frontal alien hand syndrome (AHS) presents as impulsive grasping and groping and compulsive manipulation of environmental objects that can affect the dominant or nondominant hand. A few reports have shown improvements in neuropsychological scores over time when self-restraint of the right hand AHS was enforced. A 72-year-old woman presented with right-handed involuntary instinctive grasping reactions and compulsive manipulation of tools after an infarction of the frontal lobe and corpus callosum (CC). She was diagnosed with cerebral infarction involving the anterior cerebral artery territory and a frontal variant of AHS. At AHS onset, the patient was unaware that her right hand was moving against her will; she was only aware that her right hand was moving when the therapist pointed it out to her. Later, she began to recognize that her right hand was involuntarily moving, and she could restrain the movement of her right hand with her left hand. Approximately 5 months following AHS onset, the patient could voluntarily restrain her AHS symptoms by telling her right hand not to move against her will in her head. Most neuropsychological scores improved by 5 months following AHS onset. However, the patient showed disruptions in the genu and midbody of the left cingulate cortex, as shown via diffusion tensor imaging (DTI), and the sensation of the "right hand moving by itself" remained even 5 months after AHS onset. Although damage to the CC fibers was evident on DTI at 5 months following onset, the patient exhibited no sensory deficits and demonstrated good hand ownership as well as early improvement in attention and cognitive dysfunction. Therefore, the patient recognized her AHS symptoms, which included her hand moving against her will, and was able to consciously restrain her hand movement.
额叶异己手综合征(AHS)表现为对环境物体的冲动性抓握、摸索及强迫性操作,可累及优势手或非优势手。有几份报告显示,当对右手AHS进行自我约束时,神经心理学评分会随时间改善。一名72岁女性在额叶和胼胝体(CC)梗死之后出现右手非自愿的本能抓握反应及对工具的强迫性操作。她被诊断为涉及大脑前动脉区域的脑梗死及AHS的额叶变异型。在AHS发作时,患者并未意识到自己的右手在违背其意愿地移动;只有当治疗师指给她看时,她才意识到右手在动。后来,她开始认识到自己的右手在非自愿地移动,并且能用左手抑制右手的移动。在AHS发作大约5个月后,患者能够通过在脑海中告诉右手不要违背其意愿移动来主动抑制AHS症状。AHS发作5个月后,大多数神经心理学评分有所改善。然而,弥散张量成像(DTI)显示,患者左侧扣带回皮质的膝部和中部存在破坏,并且即使在AHS发作5个月后,“右手自行移动”的感觉仍然存在。虽然在发作后5个月时,DTI显示CC纤维有明显损伤,但患者没有感觉缺陷,表现出良好的手部归属意识,并且注意力和认知功能障碍也有早期改善。因此,患者认识到了包括右手违背其意愿移动在内的AHS症状,并且能够有意识地抑制手部运动。