Department of Medical Oncology, Kyorin University Faculty of Medicine, Tokyo, Japan.
Department of Hepatobiliary and Pancreatic Oncology, National Cancer Center Hospital, Tokyo, Japan.
Oncologist. 2024 Jan 5;29(1):e97-e107. doi: 10.1093/oncolo/oyad220.
Recent studies suggest that early tumor shrinkage (ETS) and depth of response (DpR) reflect outcomes of chemotherapy in various cancers. This study evaluated the association of ETS and DpR with clinical outcomes using data from JCOG1113, which demonstrated the non-inferiority of gemcitabine plus S-1 (GS) to gemcitabine plus cisplatin (GC) for chemotherapy-naïve advanced biliary tract cancer.
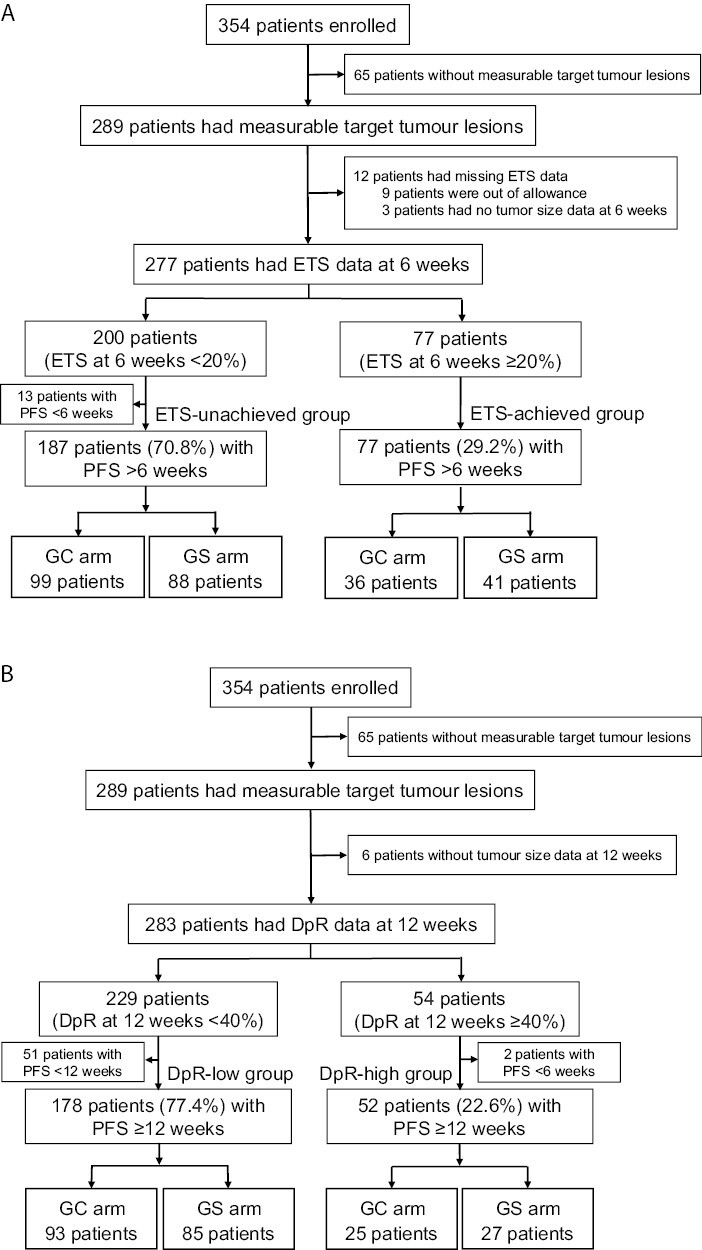
In total, 354 (289 with measurable target lesions) patients enrolled in JCOG1113 were divided into ETS-unachieved and ETS-achieved groups (≥20% tumor reduction at week 6) and DpR-low and DpR-high groups (≥40% maximum shrinkage) until 12 weeks after enrollment. The impact of ETS and DpR on survival outcome was evaluated using the multivariable Cox proportional hazard model.
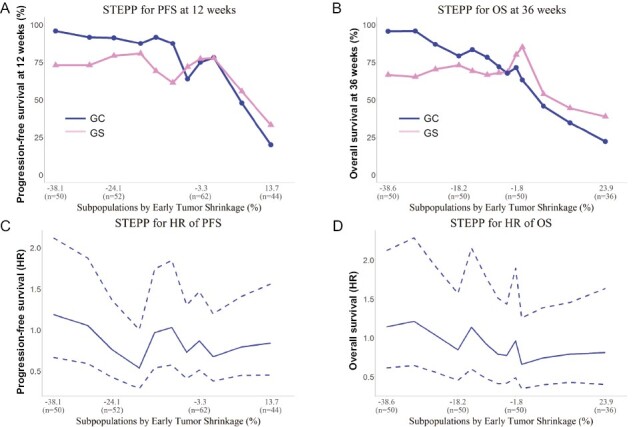
The proportions of patients in the ETS-achieved and DpR-high groups were similar between the 2 treatment arms. The hazard ratios (HRs) of progression-free survival (PFS) and overall survival (OS) for the ETS-achieved group were 0.70 (95% confidence interval (CI), 0.52-0.93) and 0.60 (95%CI, 0.44-0.81), respectively. The HRs of PFS and OS for the DpR-high group were 0.67 (95%CI, 0.48-0.94) and 0.64 (95%CI, 0.46-0.90), respectively. In the subpopulation treatment effect pattern plot analysis, most patients in the ETS-achieved group in the GC arm did not experience disease progression after 12 weeks from the landmark.
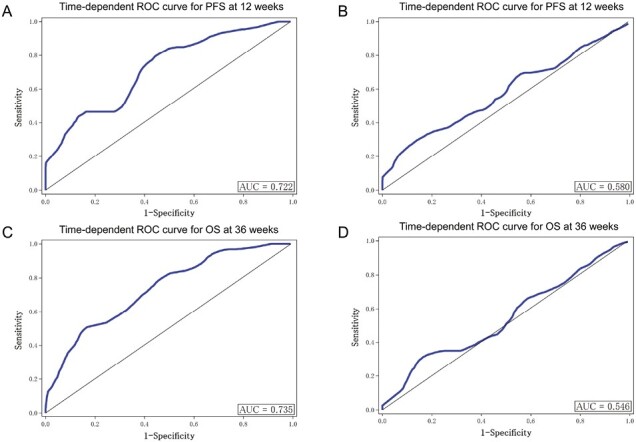
As on-treatment markers, ETS and DpR were effective tools. ETS was clinically useful, because it can be used to evaluate the outcomes of treatment early at a specific time.
最近的研究表明,早期肿瘤退缩(ETS)和深度缓解(DpR)反映了各种癌症化疗的结果。本研究使用 JCOG1113 的数据评估了 ETS 和 DpR 与临床结果的相关性,该研究表明吉西他滨联合 S-1(GS)与吉西他滨联合顺铂(GC)相比在化疗初治的晚期胆道癌中不劣效。
总共纳入了 JCOG1113 的 354 名(289 名有可测量的靶病灶)患者,根据第 6 周时 ETS 未达到和 ETS 达到(肿瘤缩小≥20%)以及 DpR 低和 DpR 高(最大缩小≥40%)分为两组,直到入组后 12 周。使用多变量 Cox 比例风险模型评估 ETS 和 DpR 对生存结果的影响。
在 2 个治疗组中,ETS 达到组和 DpR 高组的患者比例相似。在 ETS 达到组中,无进展生存期(PFS)和总生存期(OS)的风险比(HR)分别为 0.70(95%置信区间[CI],0.52-0.93)和 0.60(95%CI,0.44-0.81)。在 DpR 高组中,PFS 和 OS 的 HR 分别为 0.67(95%CI,0.48-0.94)和 0.64(95%CI,0.46-0.90)。在亚组治疗效果模式图分析中,GC 组中大多数 ETS 达到组的患者在 12 周的标记时间后没有出现疾病进展。
作为治疗中的标志物,ETS 和 DpR 是有效的工具。ETS 具有临床实用性,因为它可以在特定时间点早期评估治疗结果。