Department of Pulmonary and Critical Care Medicine, Mayo Clinic, Gonda 18-South, 200 1st St SW, Rochester, MN, 55905, USA.
Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Gonda 18-South, 200 1st St SW, Rochester, MN, 55905, USA.
BMC Pulm Med. 2023 Aug 2;23(1):281. doi: 10.1186/s12890-023-02565-7.
Create a timeline of diagnosis and treatment for IPF in the US.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective analysis was performed in collaboration with the OptumLabs Data Warehouse using an administrative claims database of Medicare Fee for Service beneficiaries. Adults 50 and over with IPF were included (2014 to 2019).
To focus on IPF, the following diagnoses were excluded: post-inflammatory fibrosis, hypersensitivity pneumonitis, rheumatoid arthritis, sarcoidosis, scleroderma, and connective tissue disease.
Data were collected from periods prior, during, and following initial clinical diagnosis of IPF. This included prior respiratory diagnoses, number of respiratory-related hospitalizations, anti-fibrotic and oxygen use, and survival.
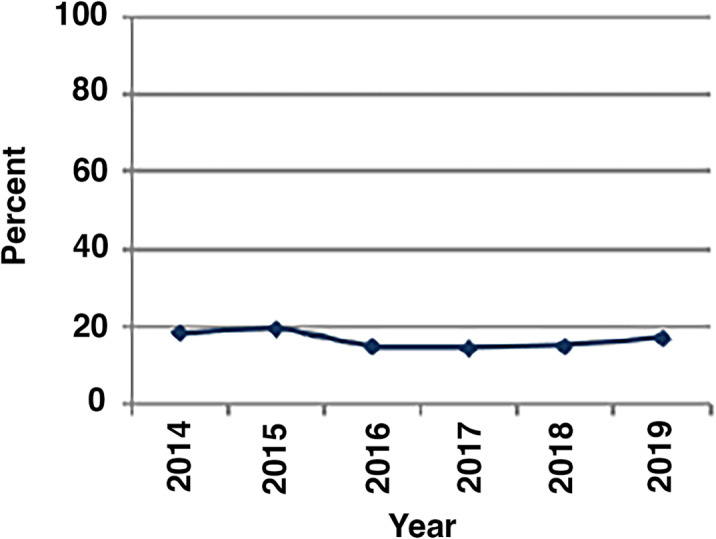
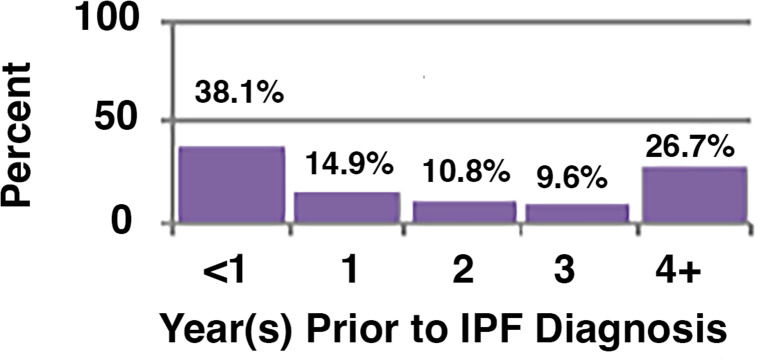
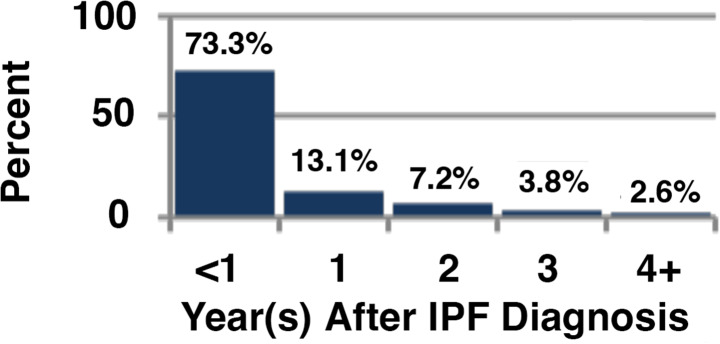
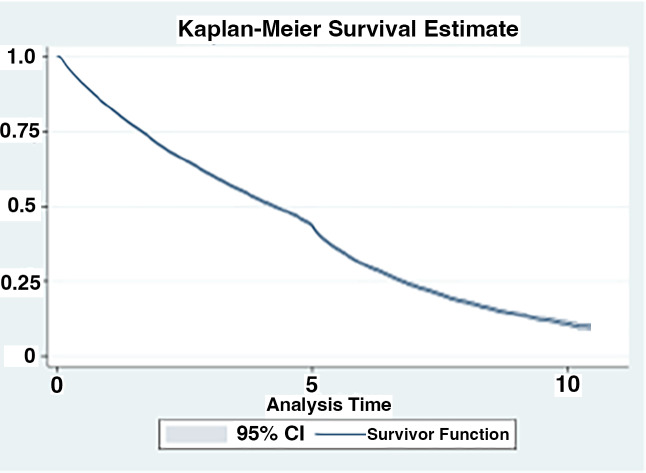
A total of 44,891 with IPF were identified. The most common diagnoses prior to diagnosis of IPF were upper respiratory infections (47%), acute bronchitis (13%), other respiratory disease (10%), chronic obstructive pulmonary disease and bronchiectasis (7%), and pneumonia (6%). The average time to a diagnosis of IPF was 2.7 years after initial respiratory diagnosis. Half of patients had two or more respiratory-related hospitalizations prior to IPF diagnosis. Also, 37% of patients were prescribed oxygen prior to diagnosis of IPF. These observations suggest delayed diagnosis. We also observed only 10.4% were treated with anti-fibrotics. Overall survival declined each year after diagnosis with median survival of 2.80 years.
Our retrospective cohort demonstrates that IPF is often diagnosed late, usually preceded by other respiratory diagnoses and hospitalizations. Use of available therapies is low and outcomes remain poor.
在美国建立特发性肺纤维化(IPF)的诊断和治疗时间轴。
设计、设置和参与者:本研究通过使用医疗保险按服务收费受益人的 OptumLabs 数据仓库进行回顾性分析,合作进行了一项回顾性分析。纳入年龄在 50 岁及以上的 IPF 成人患者(2014 年至 2019 年)。
为了专注于 IPF,排除了以下诊断:炎症后纤维化、过敏性肺炎、类风湿性关节炎、结节病、硬皮病和结缔组织疾病。
从 IPF 初始临床诊断之前、期间和之后的时间段收集数据。这包括先前的呼吸道诊断、呼吸道相关住院次数、抗纤维化和氧气使用情况以及生存率。
共确定了 44891 例 IPF 患者。在诊断为 IPF 之前,最常见的诊断是上呼吸道感染(47%)、急性支气管炎(13%)、其他呼吸道疾病(10%)、慢性阻塞性肺疾病和支气管扩张(7%)以及肺炎(6%)。从首次呼吸道诊断到 IPF 诊断的平均时间为 2.7 年。一半的患者在 IPF 诊断前有两次或更多次呼吸道相关住院治疗。此外,在诊断为 IPF 之前,有 37%的患者接受了氧气治疗。这些观察结果表明存在诊断延迟。我们还观察到,只有 10.4%的患者接受了抗纤维化治疗。诊断后,患者的总体生存率每年都在下降,中位生存时间为 2.80 年。
我们的回顾性队列研究表明,IPF 通常诊断较晚,通常先于其他呼吸道诊断和住院治疗。可用疗法的使用率较低,预后仍然较差。