Lei Jie, Zhao Jinbo, Gong Li, Ni Yunfeng, Zhou Yongan, Tian Feng, Liu Honggang, Gu Zhongping, Huang Lijun, Lu Qiang, Wang Xiaoping, Sun Jianyong, Yang Ende, Wang Tao, Zhong Daixing, Wang Jian, Zhao Zhengwei, Liu Zhigang, Wang Cheng, Wang Xiaojing, Lei Guangyan, Yan Xiaolong, Jiang Tao
Department of Thoracic Surgery, The Second Affiliated Hospital of Air Force Medical University, Xi'an, China.
Department of Pathology, The Second Affiliated Hospital of Air Force Medical University, Xi'an, China.
JAMA Oncol. 2023 Oct 1;9(10):1348-1355. doi: 10.1001/jamaoncol.2023.2751.
The benefit of neoadjuvant camrelizumab plus chemotherapy for resectable stage IIIA or IIIB non-small cell lung cancer (NSCLC) remains unknown.
To assess the efficacy and safety of neoadjuvant camrelizumab plus chemotherapy vs chemotherapy alone for patients with resectable stage IIIA or IIIB NSCLC.
DESIGN, SETTING, AND PARTICIPANTS: In this randomized phase 2 clinical trial conducted at 2 hospitals in China, patients aged 18 to 70 years with resectable stage IIIA or IIIB (T3N2) NSCLC were enrolled between April 7, 2020, and January 12, 2022.
Patients were randomly assigned to receive 3 cycles of camrelizumab (200 mg) plus chemotherapy (nab-paclitaxel, 130 mg/m2, and platinum [cisplatin, 75 mg/m2; carboplatin, area under the curve, 5; or nedaplatin, 100 mg/m2]) or chemotherapy alone, followed by surgery after 4 to 6 weeks.
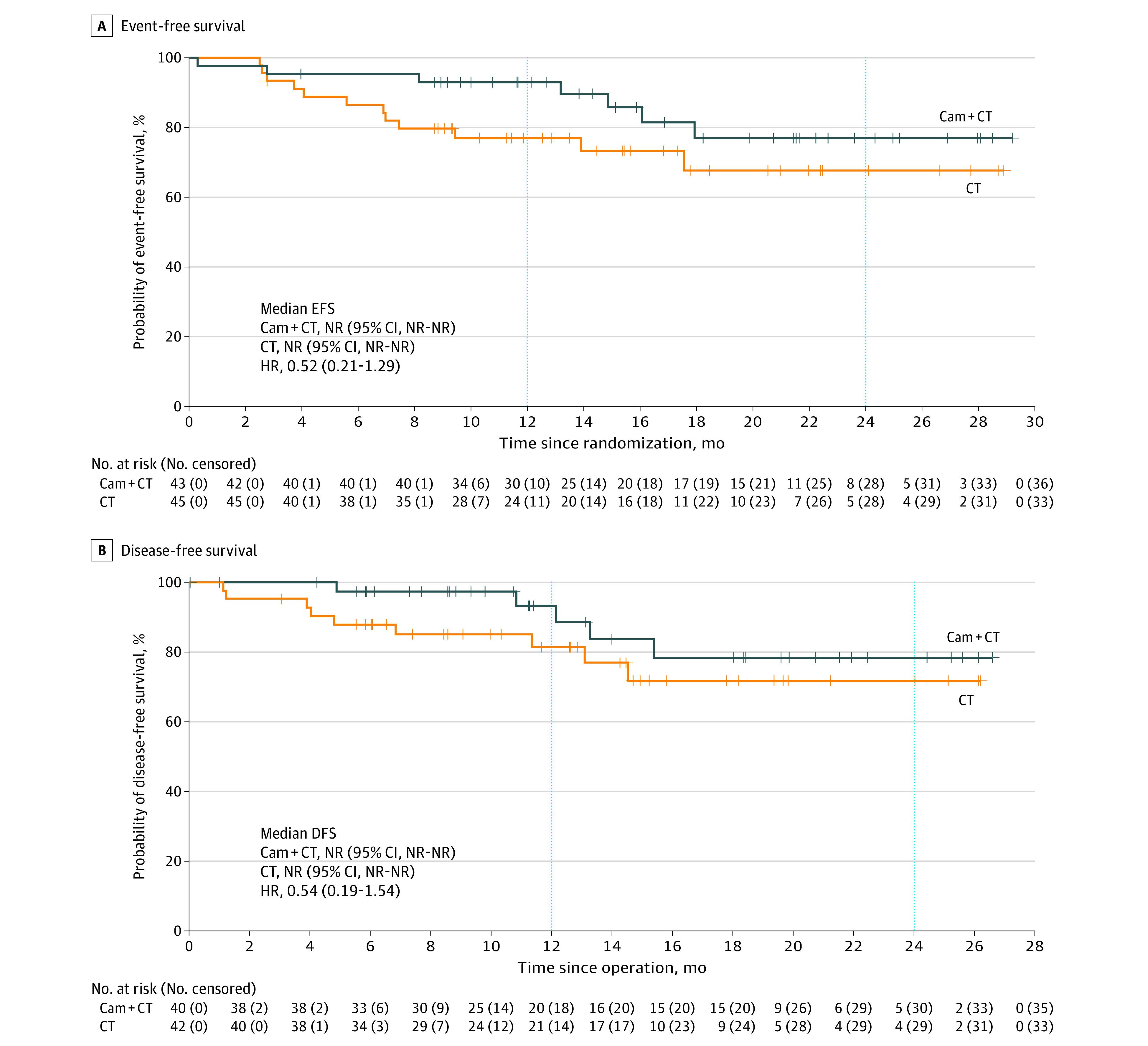
The primary end point was the pathologic complete response (pCR) rate. Secondary end points included the major pathologic response (MPR) rate, objective response rate (ORR), event-free survival (EFS), and safety. Disease-free survival (DFS, defined as the time from surgery to disease recurrence or death from any cause) was analyzed post hoc. Efficacy was assessed on a modified intention-to-treat basis.
Ninety-four Chinese patients were randomized, and 88 (93.6%; median age, 61 years [IQR, 54-65 years]; 74 men [84.1%]) received allocated neoadjuvant treatment (43 received camrelizumab plus chemotherapy, and 45 received chemotherapy alone). Among these 88 patients, the pCR rate was 32.6% (14 of 43; 95% CI, 19.1%-48.5%) with camrelizumab plus chemotherapy vs 8.9% (4 of 45; 95% CI, 2.5%-21.2%) with chemotherapy alone (odds ratio, 4.95; 95% CI, 1.35-22.37; P = .008). The MPR rates were 65.1% (95% CI, 49.1%-79.0%) with camrelizumab plus chemotherapy and 15.6% (95% CI, 6.5%-29.5%) with chemotherapy alone. The radiographic ORRs were 72.1% (95% CI, 56.3%-84.7%) with camrelizumab plus chemotherapy and 53.3% (95% CI, 37.9%-68.3%) with chemotherapy alone. With a median follow-up of 14.1 months (IQR, 9.2-20.9 months), the median EFS and DFS were not reached in either group. The most common neoadjuvant treatment-related adverse events of grade 3 or higher were decreased white blood cell count (6 of 43 [14.0%] in the camrelizumab plus chemotherapy group vs 2 of 45 [4.4%] in the chemotherapy group) and decreased neutrophil count (3 of 43 [7.0%] in the camrelizumab plus chemotherapy group vs 5 of 45 [11.1%] in the chemotherapy group). No treatment-related deaths were reported.
This randomized clinical trial found that among patients with resectable stage IIIA or IIIB (T3N2) NSCLC, camrelizumab plus chemotherapy, compared with chemotherapy alone, significantly improved the pCR rate with manageable toxic effects.
ClinicalTrials.gov Identifier: NCT04338620.
对于可切除的IIIA期或IIIB期非小细胞肺癌(NSCLC),新辅助卡瑞利珠单抗联合化疗的益处尚不清楚。
评估新辅助卡瑞利珠单抗联合化疗与单纯化疗相比,对可切除的IIIA期或IIIB期NSCLC患者的疗效和安全性。
设计、地点和参与者:在这项在中国两家医院进行的随机2期临床试验中,年龄在18至70岁、患有可切除的IIIA期或IIIB期(T3N2)NSCLC的患者于2020年4月7日至2022年1月12日入组。
患者被随机分配接受3个周期的卡瑞利珠单抗(200mg)联合化疗(白蛋白结合型紫杉醇,130mg/m²,和顺铂[顺铂,75mg/m²;卡铂,曲线下面积5;或奈达铂,100mg/m²])或单纯化疗,4至6周后进行手术。
主要终点是病理完全缓解(pCR)率。次要终点包括主要病理缓解(MPR)率、客观缓解率(ORR)、无事件生存期(EFS)和安全性。无病生存期(DFS,定义为从手术到疾病复发或因任何原因死亡的时间)进行事后分析。疗效在改良意向性分析基础上进行评估。
94例中国患者被随机分组,88例(93.6%;中位年龄61岁[四分位间距,54 - 65岁];74例男性[84.1%])接受了分配的新辅助治疗(43例接受卡瑞利珠单抗联合化疗,45例接受单纯化疗)。在这88例患者中,卡瑞利珠单抗联合化疗组的pCR率为32.6%(43例中的14例;95%CI,19.1% - 48.5%),而单纯化疗组为8.9%(45例中的4例;95%CI,2.5% - 21.2%)(优势比,4.95;95%CI,1.35 - 22.37;P = 0.008)。MPR率在卡瑞利珠单抗联合化疗组为65.1%(95%CI,49.1% - 79.0%),单纯化疗组为15.6%(95%CI,6.5% - 29.5%)。影像学ORR在卡瑞利珠单抗联合化疗组为72.1%(95%CI,56.3% - 84.7%),单纯化疗组为53.3%(95%CI,37.9% - 68.3%)。中位随访14.1个月(四分位间距,9.2 - 20.9个月),两组的中位EFS和DFS均未达到。最常见的3级或更高等级的新辅助治疗相关不良事件是白细胞计数减少(卡瑞利珠单抗联合化疗组43例中的6例[14.0%],化疗组45例中的2例[4.4%])和中性粒细胞计数减少(卡瑞利珠单抗联合化疗组43例中的3例[7.0%],化疗组45例中的5例[11.1%])。未报告与治疗相关的死亡。
这项随机临床试验发现,在可切除的IIIA期或IIIB期(T3N2)NSCLC患者中,与单纯化疗相比,卡瑞利珠单抗联合化疗显著提高了pCR率,且毒性效应可控。
ClinicalTrials.gov标识符:NCT04338620。