Department of Obstetrics and Gynecology, Nihon University Hospital, 1-6 Kanda Surugadai Chiyoda-ku, Tokyo, 101-8309, Japan.
Department of Obstetrics and Gynecology, Nihon University School of Medicine, 30-1 Oyaguchi Kami-cho, Itabashi-ku, Tokyo, 173-8610, Japan.
BMC Womens Health. 2023 Aug 3;23(1):406. doi: 10.1186/s12905-023-02539-1.
Uterine diverticulum is classified into congenital and acquired types. The acquired type is caused by caesarean scar syndrome, which occurs after caesarean section. There are no detailed reports on diverticulum after enucleation of uterine fibroids. Most cases are treated with hysteroscopy or laparoscopy, but a management consensus is lacking. We treated a patient with a uterine diverticulum that had formed after uterine fibroid enucleation by combining hysteroscopic and laparoscopic treatments.
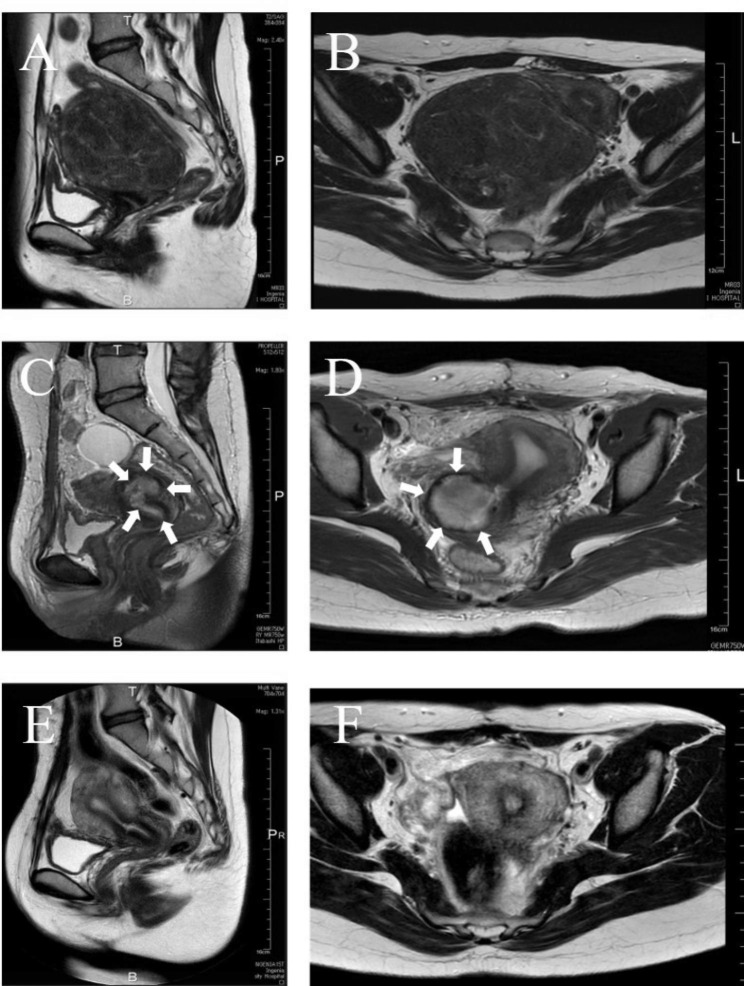
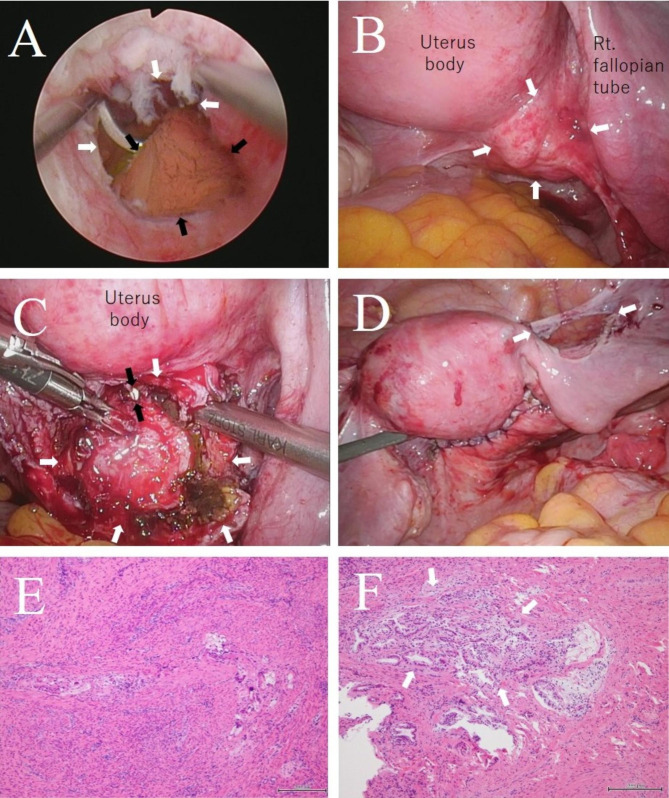
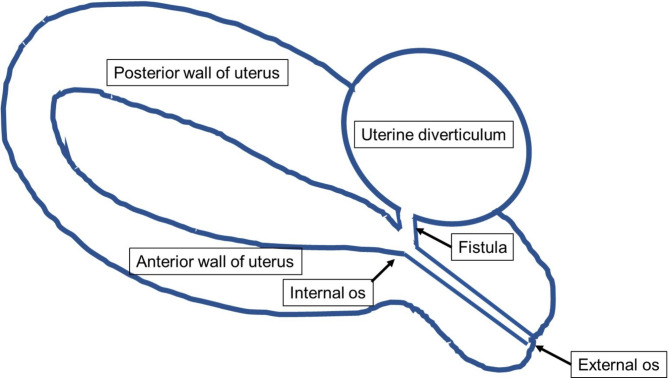
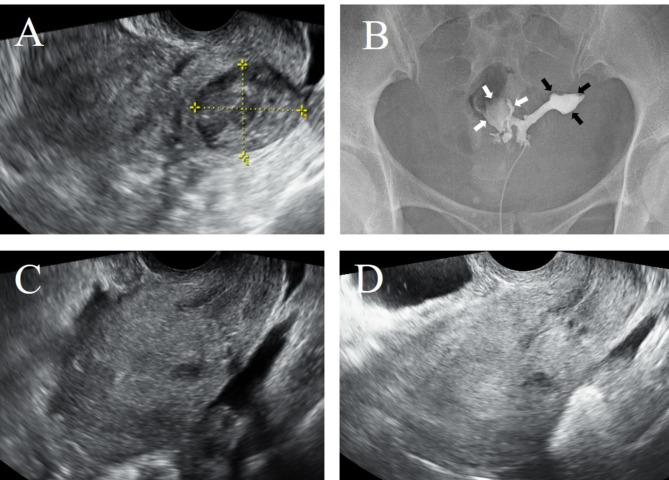
The patient was a 37-year-old Japanese woman, G1P0. A previous doctor had performed abdominal uterine myomectomy for a pedunculated subserosal uterine fibroid on the right side of the posterior wall of the uterus near the internal cervical os. Menstruation resumed postoperatively, but a small amount of dark-red bleeding persisted. MRI two months after the myomectomy revealed a diverticulum-like structure 3 cm in diameter, communicating with the uterine lumen, on the right side of the posterior wall of the uterus. Under suspicion of uterine diverticulum after uterine fibroid enucleation, the patient sought treatment at our hospital approximately four months after the myomectomy. Through a flexible hysteroscope, a 5-mm-diameter fistula was observed in the posterior wall of the uterus, and a contrast-enhanced pocket, measuring approximately 3 cm, was located behind it. Uterine diverticulum following enucleation of a uterine fibroid was diagnosed, and surgery was thus deemed necessary. The portion entering the fistula on the internal cervical os side was resected employing a hysteroscope. Intra-abdominal findings included a 4-cm mass lesion on the posterior wall on the right side of the uterus. The mass was opened, and the cyst capsule was removed. A 5-mm fistula was detected and closed with sutures. Resuturing was not performed after dissection of the right round ligament due to tension. The postoperative course has been good to date, with no recurrence.
Uterine diverticula after myomectomy may be treated with a combined laparoscopic and hysteroscopic approach, similar to caesarean scar syndrome.
子宫憩室分为先天性和后天性两种类型。后天性憩室是由剖宫产瘢痕综合征引起的,发生于剖宫产术后。关于子宫肌瘤剔除术后憩室的报道较少。大多数情况下采用宫腔镜或腹腔镜治疗,但缺乏管理共识。我们采用宫腔镜联合腹腔镜治疗了 1 例子宫肌瘤剔除术后子宫憩室患者。
患者为 37 岁日本女性,G1P0。既往医生曾行经腹子宫肌瘤剔除术,剔除位于子宫颈口内后侧右后壁的带蒂浆膜下子宫肌瘤。术后月经恢复,但仍有少量暗红色出血。子宫肌瘤剔除术后 2 个月行 MRI 检查发现子宫右后壁直径 3cm 的憩室样结构,与宫腔相通。考虑为子宫肌瘤剔除术后子宫憩室,患者于术后约 4 个月就诊于我院。经软性宫腔镜检查,发现子宫后壁有 5mm 直径的瘘口,其后有一增强的囊袋,大小约 3cm。诊断为子宫肌瘤剔除术后子宫憩室,需要手术治疗。采用宫腔镜切除子宫颈口内后侧进入瘘口的部分。腹腔内发现右侧子宫后壁有 4cm 大小的肿块。切开肿块,切除囊壁。发现 5mm 瘘口,用缝线缝合关闭。由于右侧圆韧带张力较大,分离后未进行再次缝合。术后恢复良好,无复发。
与剖宫产瘢痕综合征类似,对于子宫肌瘤剔除术后的子宫憩室,可以采用腹腔镜联合宫腔镜的方法进行治疗。