Surveillance & Health Equity Science, American Cancer Society, Atlanta, Georgia.
Department of Medicine, Brookdale University Hospital and Medical Center, Brooklyn, New York.
JAMA Netw Open. 2023 Aug 1;6(8):e2327429. doi: 10.1001/jamanetworkopen.2023.27429.
Comprehensive data for racial and ethnic disparities after second primary cancers (SPCs) are lacking despite the growing burden of SPCs.
To quantify racial and ethnic disparities in survival among persons with SPCs.
DESIGN, SETTING, AND PARTICIPANTS: This population-based, retrospective cohort study used data from 18 Surveillance, Epidemiology, and End Results registries in the US for persons diagnosed with the most common SPCs at age 20 years or older from January 1, 2000, to December 31, 2013 (with follow-up through December 31, 2018). Data were analyzed between January and April 2023.
Race and ethnicity (Hispanic, non-Hispanic Asian or Pacific Islander, non-Hispanic Black, and non-Hispanic White).
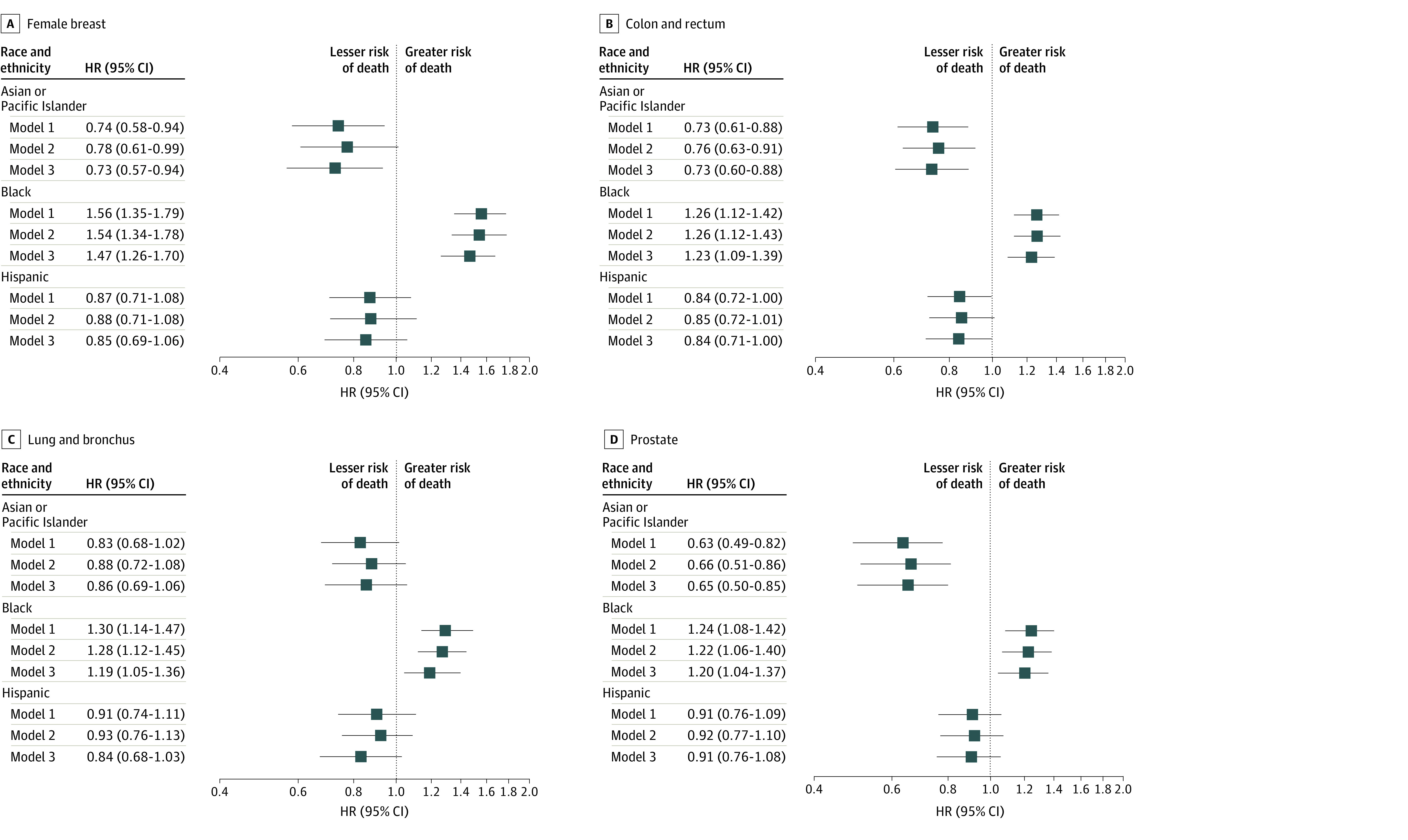
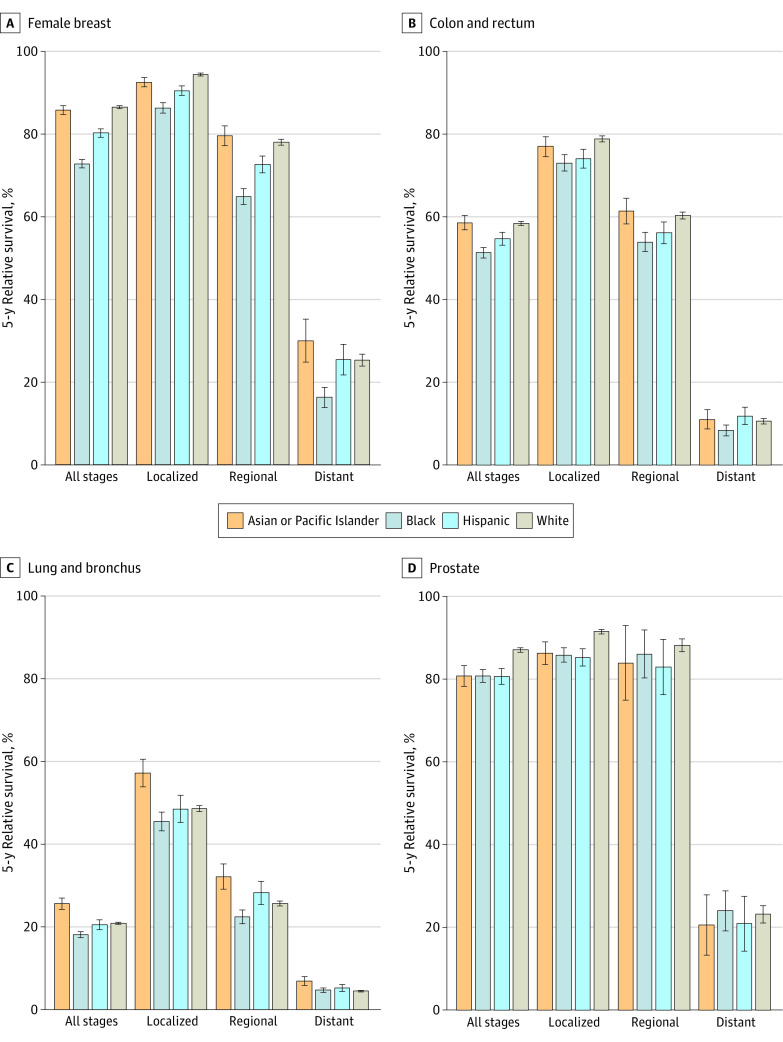
The main outcomes were 5-year relative survival and cause-specific survival. Cause-specific hazard ratios (HRs) were calculated for death from cancer or cardiovascular disease (CVD) in each racial and ethnic minority population compared with the White population overall and stratified by SPC type, with adjustment for sex, year and age at SPC diagnosis, and prior cancer type and stage (baseline model) and additionally for county attributes (household income, urbanicity), SPC characteristics (stage, subtype), and treatment.
Among 230 370 persons with SPCs (58.4% male), 4.5% were Asian or Pacific Islander, 9.6% were Black, 6.4% were Hispanic, and 79.5% were White. A total of 109 757 cancer-related deaths (47.6%) and 18 283 CVD-related deaths (7.9%) occurred during a median follow-up of 54 months (IQR, 12-93 months). In baseline models, compared with the White population, the risk of cancer-related death overall was higher in the Black (HR, 1.21; 95% CI, 1.18-1.23) and Hispanic (HR, 1.10; 95% CI, 1.07-1.13) populations but lower in the Asian or Pacific Islander population (HR, 0.93; 95% CI, 0.90-0.96). When stratified by 13 SPC types, the risk of cancer-related death was higher for 10 SPCs in the Black population, with the highest HR for uterine cancer (HR, 1.87; 95% CI, 1.63-2.15), and for 7 SPCs in the Hispanic population, most notably for melanoma (HR, 1.46; 95% CI, 1.21-1.76). For CVD-related death, the overall HR was higher in the Black population (HR, 1.41; 95% CI, 1.34-1.49), with elevated risks evident for 11 SPCs, but lower in the Asian or Pacific Islander (HR, 0.75; 95% CI, 0.69-0.81) and Hispanic (HR, 0.90; 95% CI, 0.84-0.96) populations than in the White population. After further adjustments for county attributes and SPC characteristics and treatment, HRs were reduced for cancer-related death and for CVD-related death and associations in the same direction remained.
In this cohort study of SPC survivors, the Black population had the highest risk of both death from cancer and death from CVD, and the Hispanic population had a higher risk of death from cancer than the White population. Attenuations in HRs after adjustment for potentially modifiable factors highlight opportunities to reduce survival disparities among persons with multiple primary cancers.
尽管二次原发性癌症(SPCs)的负担不断增加,但缺乏有关种族和族裔差异的综合数据。
量化 SPC 患者生存中的种族和族裔差异。
设计、地点和参与者:这是一项基于人群的回顾性队列研究,使用了美国 18 个监测、流行病学和最终结果登记处的数据,纳入了 20 岁及以上首次诊断为最常见 SPCs 的患者,随访至 2018 年 12 月 31 日(数据分析于 2023 年 1 月至 4 月进行)。
种族和族裔(西班牙裔、非西班牙裔亚裔或太平洋岛民、非西班牙裔黑人和非西班牙裔白人)。
主要结局是 5 年相对生存率和病因特异性生存率。计算了每种少数族裔人群与白人总体相比的癌症或心血管疾病(CVD)死亡的病因特异性风险比(HR),并按 SPC 类型分层,调整了性别、SPC 诊断时的年份和年龄以及先前癌症类型和分期(基线模型),并进一步调整了县属性(家庭收入、城市性)、SPC 特征(分期、亚型)和治疗。
在 230370 名患有 SPCs 的患者中(58.4%为男性),4.5%为亚裔或太平洋岛民,9.6%为黑人,6.4%为西班牙裔,79.5%为白人。在中位随访 54 个月(IQR,12-93 个月)期间,共发生 109757 例与癌症相关的死亡(47.6%)和 18283 例与 CVD 相关的死亡(7.9%)。在基线模型中,与白人相比,黑人(HR,1.21;95%CI,1.18-1.23)和西班牙裔(HR,1.10;95%CI,1.07-1.13)人群的癌症相关死亡风险更高,但亚裔或太平洋岛民(HR,0.93;95%CI,0.90-0.96)人群的风险较低。按 13 种 SPC 类型分层时,黑人人群中有 10 种 SPC 的癌症相关死亡风险更高,其中子宫癌的 HR 最高(HR,1.87;95%CI,1.63-2.15),而在西班牙裔人群中,有 7 种 SPC 的癌症相关死亡风险更高,最显著的是黑色素瘤(HR,1.46;95%CI,1.21-1.76)。对于 CVD 相关死亡,黑人人群的总体 HR 更高(HR,1.41;95%CI,1.34-1.49),11 种 SPC 的风险升高,但亚裔或太平洋岛民(HR,0.75;95%CI,0.69-0.81)和西班牙裔(HR,0.90;95%CI,0.84-0.96)人群的风险低于白人。进一步调整县属性和 SPC 特征以及治疗后,癌症相关死亡和 CVD 相关死亡的 HR 降低,且相关性保持不变。
在这项 SPC 幸存者队列研究中,黑人人群的癌症和 CVD 死亡风险最高,而西班牙裔人群的癌症死亡风险高于白人人群。调整潜在可改变因素后 HR 的衰减突出了减少多重原发性癌症患者生存差异的机会。