Eichinger Martin, Ploner Martin, Degenhart Gerald, Rudisch Ansgar, Smekal Vinzenz, Attal René, Mayr Raul
Department of Orthopedics and Traumatology, a.ö. Bezirkskrankenhaus St. Johann in Tirol, Tirol, Austria.
Department of Orthopedics and Traumatology, Medical University of Innsbruck, Anichstrasse 35, 6020, Innsbruck, Austria.
Arch Orthop Trauma Surg. 2023 Nov;143(11):6707-6718. doi: 10.1007/s00402-023-05001-x. Epub 2023 Aug 5.
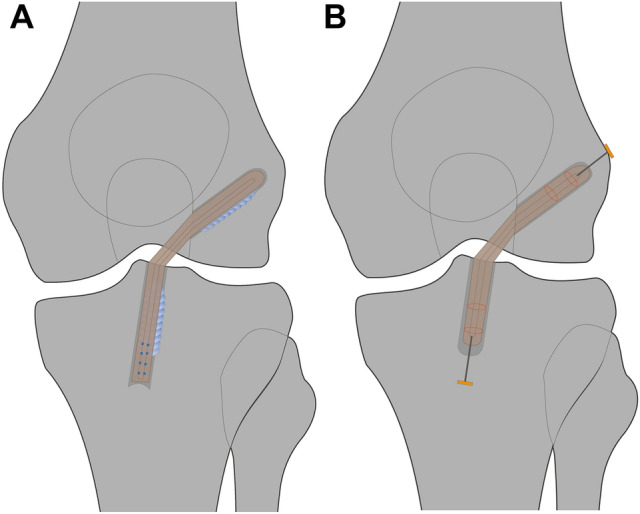
The aim of the present study was to examine tunnel widening and clinical outcomes after anterior cruciate ligament reconstruction (ACLR) using two different fixation methods: aperture fixation with biodegradable interference screws versus all-inside ACLR with suspensory cortical buttons.
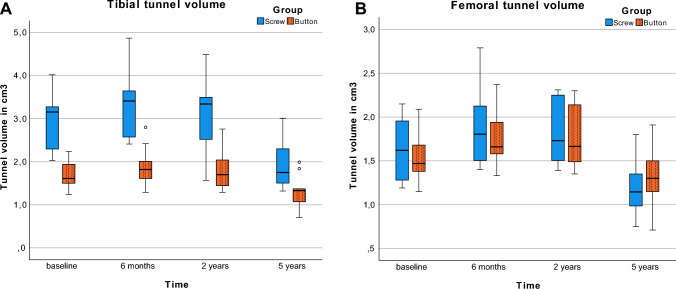
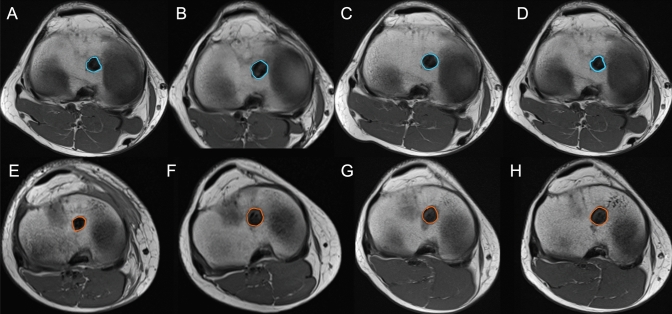
Tunnel widening was assessed using volumetric and diameter measurements on magnetic resonance imaging (MRI) scans directly after surgery, as well as 6 months and 2 and 5 years postoperatively. Clinical outcomes were assessed after 5 years with instrumented tibial anteroposterior translation measurement (KT-1000), single-leg hop testing, and the IKDC, Lysholm, and Tegner activity scores.
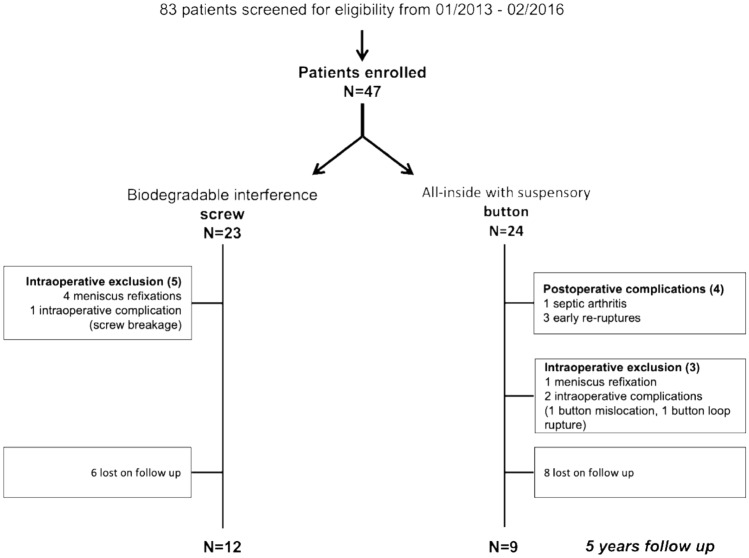
At the final follow-up, the study population consisted of 21 patients, 12 of whom underwent screw fixation and 9 of whom had button fixation. 3 patients with all-inside ACLR had sustained early repeat ruptures within 6 months after surgery and had to be excluded from the further analysis. With screw fixation, the tibial tunnel volume changed significantly more over time compared to all-inside button fixation, with a larger initial increase at 6 months (from postoperative 2.9 ± 0.2 to 3.3 ± 0.2 cm at 6 months versus 1.7 ± 0.1 to 1.9 ± 0.2 cm) and a greater final decrease over 2-5 years postoperatively (from 3.1 ± 0.2 to 1.9 ± 0.2 cm versus 1.8 ± 0.2 ± 0.1 to 1.3 ± 0.1 cm) (P < 0.001). The femoral tunnel volume remained comparable between the two groups throughout the follow-up period, with an initial 1.6 ± 0.1 cm in both groups and 1.2 ± 0.1 vs. 1.3 ± 0.1 after 5 years in the screw and button groups, respectively (P ≥ 0.314). The maximum tibial and femoral tunnel diameters were significantly larger with screw fixation at all four time points. Tibial diameters measured 11.1 ± 0.2, 12.3 ± 0.3, 12.3 ± 0.4, and 11.2 ± 0.4 mm in the screw group versus 8.1 ± 0.3, 8.9 ± 0.3, 9.1 ± 0.4 and 8.2 ± 0.5 mm in the button group (P < 0.001). Femoral diameters measured 8.6 ± 0.2, 10.5 ± 0.4, 10.2 ± 0.3, and 8.9 ± 0.3 versus 7.3 ± 0.3, 8.4 ± 0.4, 8.4 ± 0.3, 7.5 ± 0.3, respectively (P ≤ 0.007). Four patients (33%) in the screw group exceeded a diameter of 12 mm on the tibial side after 5 years versus none in the button group (not significant, P = 0.104). Tibial anteroposterior translation measurement with KT-1000 after 5 years was 2.3 ± 2.4 mm in the screw group versus 3.2 ± 3.5 mm in the button group (not significant, P = 0.602). There were no significant differences between the groups in any of the other clinical outcomes.
Tibial tunnels in ACLR with screw fixation were associated with a larger increase in tunnel volume within the first 2 years and a greater decrease up to 5 years after surgery, while femoral tunnel volumes did not differ significantly. On the tibial side, the need for staged revision ACLR may be greater after biodegradable interference screw fixation if repeat ruptures occur, especially within the first 2 years after primary ACLR. Concerns may remain regarding a higher graft failure rate with all-inside ACLR.
II.
NCT01755819.
本研究旨在比较两种不同固定方法在前交叉韧带重建(ACLR)术后的隧道扩大情况及临床疗效:使用可生物降解挤压螺钉的骨隧道固定法与采用悬吊皮质纽扣的全内置ACLR法。
通过术后即刻、术后6个月以及术后2年和5年的磁共振成像(MRI)扫描,采用容积测量和直径测量评估隧道扩大情况。术后5年,通过仪器测量胫骨前后向平移(KT - 1000)、单腿跳测试以及IKDC、Lysholm和Tegner活动评分评估临床疗效。
在最终随访时,研究对象包括21例患者,其中12例行螺钉固定,9例行纽扣固定。3例接受全内置ACLR的患者在术后6个月内早期再次发生断裂,因此被排除在进一步分析之外。与全内置纽扣固定相比,螺钉固定时胫骨隧道容积随时间变化更为显著,术后6个月时初始增加幅度更大(术后2.9±0.2至6个月时3.3±0.2 cm,而纽扣固定组为1.7±0.1至1.9±0.2 cm),术后2 - 5年最终减小幅度更大(从3.1±0.2至1.9±0.2 cm,纽扣固定组为1.8±0.2±0.1至1.3±0.1 cm)(P < 0.001)。在整个随访期间,两组股骨隧道容积相当,两组初始均为1.6±0.1 cm,螺钉组和纽扣组术后5年分别为1.2±0.1和1.3±0.1 cm(P≥0.314)。在所有四个时间点,螺钉固定时胫骨和股骨隧道的最大直径均显著更大。螺钉组胫骨直径分别为11.1±0.2、12.3±0.3、12.3±0.4和11.2±0.4 mm,纽扣组为8.1±0.3、8.9±0.3、9.1±0.4和8.2±0.5 mm(P < 0.001)。股骨直径分别为8.6±0.2、10.5±0.4、10.2±0.3和8.9±0.3,纽扣组分别为7.3±0.3、8.4±0.4、8.4±0.3和7.5±0.3(P≤0.007)。5年后,螺钉组4例患者(33%)胫骨侧直径超过12 mm,纽扣组无此情况(无显著性差异,P = 0.104)。术后5年,螺钉组KT - 1000测量的胫骨前后向平移为2.3±2.4 mm,纽扣组为3.2±3.5 mm(无显著性差异,P = 0.602)。在其他任何临床疗效方面,两组之间均无显著差异。
采用螺钉固定的ACLR中,胫骨隧道在术后前2年容积增加更大,术后5年减小幅度更大,而股骨隧道容积无显著差异。在胫骨侧,如果发生再次断裂,尤其是在初次ACLR后的前2年内,采用可生物降解挤压螺钉固定后可能更需要分期进行ACLR翻修。对于全内置ACLR较高的移植物失败率可能仍存在担忧。
II。
NCT01755819。