Basu Biswanath, Erdmann Stella, Sander Anja, Mahapatra Tapan Kumar Sinha, Meis Jan, Schaefer Franz
Division of Pediatric Nephrology, Department of Pediatrics, Nilratan Sircar Medical College and Hospital, Kolkata, India.
Institute of Medical Biometry, University of Heidelberg, Heidelberg, Germany.
Kidney Int Rep. 2023 May 29;8(8):1575-1584. doi: 10.1016/j.ekir.2023.05.022. eCollection 2023 Aug.
In the Rituximab for Relapse Prevention in Nephrotic Syndrome (RITURNS) trial, we demonstrated superior efficacy of single-course rituximab over maintenance tacrolimus in preventing relapses in children with steroid dependent nephrotic syndrome (SDNS) during a 1-year observation. Here we present the long-term outcomes of all 117 trial completers, who were followed up for another 2 years.
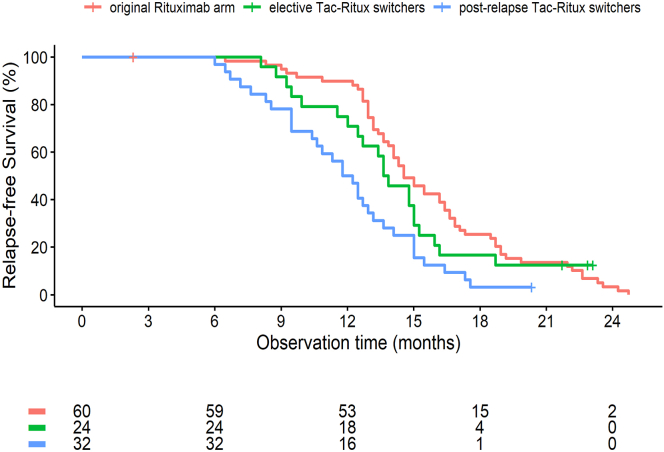
Relapsing patients in the rituximab arm received a second course of rituximab, either with ( = 44) or without mycophenolate mofetil (MMF) cotreatment ( = 15). In the tacrolimus arm, second line rituximab monotherapy was initiated after relapses ( = 32) or electively ( = 24).
All 12-month relapse-free patients in the rituximab arm relapsed in the second postexposure year, resulting in similar median relapse-free survival times in the 2 trial arms (62 vs. 59 weeks). Second line rituximab in the tacrolimus arm was less effective than first-line therapy in patients switched to rituximab following a relapse (relapse-free survival 55 vs. 63 weeks, < 0.01). B-cell counts 6 months post-rituximab predicted relapse risk both for first and second line therapy. MMF cotreatment yielded much improved 2-year relapse-free survival as compared to rituximab monotherapy (67% vs. 9%, < 0.0001). Higher grade 2 adverse event rates were observed post-rituximab versus on tacrolimus (0.87 vs. 0.53 per year).
The superior therapeutic effect of rituximab in SDNS vanishes during the second year post-exposure. Rituximab appears to yield longer remission when applied as first line as compared to second line therapy. Maintenance MMF following rituximab induces long-term disease remission.
在利妥昔单抗预防肾病综合征复发(RITURNS)试验中,我们证明了在1年观察期内,单疗程利妥昔单抗在预防激素依赖型肾病综合征(SDNS)患儿复发方面优于维持性他克莫司。在此,我们报告了全部117名试验完成者的长期结果,他们又接受了2年的随访。
利妥昔单抗组中复发的患者接受了第二疗程的利妥昔单抗治疗,其中44例联合霉酚酸酯(MMF)共同治疗,15例未联合MMF治疗。在他克莫司组中,复发后(32例)或选择性地(24例)开始二线利妥昔单抗单药治疗。
利妥昔单抗组所有12个月无复发的患者在暴露后的第二年都复发了,导致两个试验组的无复发生存时间中位数相似(62周对59周)。他克莫司组二线利妥昔单抗在复发后改用利妥昔单抗的患者中疗效不如一线治疗(无复发生存时间55周对63周,P<0.01)。利妥昔单抗治疗6个月后的B细胞计数可预测一线和二线治疗的复发风险。与利妥昔单抗单药治疗相比,MMF共同治疗使2年无复发生存率有了显著提高(67%对9%,P<0.0001)。与他克莫司治疗相比,利妥昔单抗治疗后观察到更高等级的2级不良事件发生率(每年0.87对0.53)。
利妥昔单抗在SDNS中的卓越治疗效果在暴露后的第二年消失。与二线治疗相比,利妥昔单抗作为一线治疗似乎能产生更长时间的缓解。利妥昔单抗后维持MMF可诱导疾病长期缓解。