Viral Hepatitis Clinical Research Program (VHCRP), The Kirby Institute, UNSW, Sydney, Australia.
J Viral Hepat. 2023 Dec;30(12):926-938. doi: 10.1111/jvh.13881. Epub 2023 Aug 8.
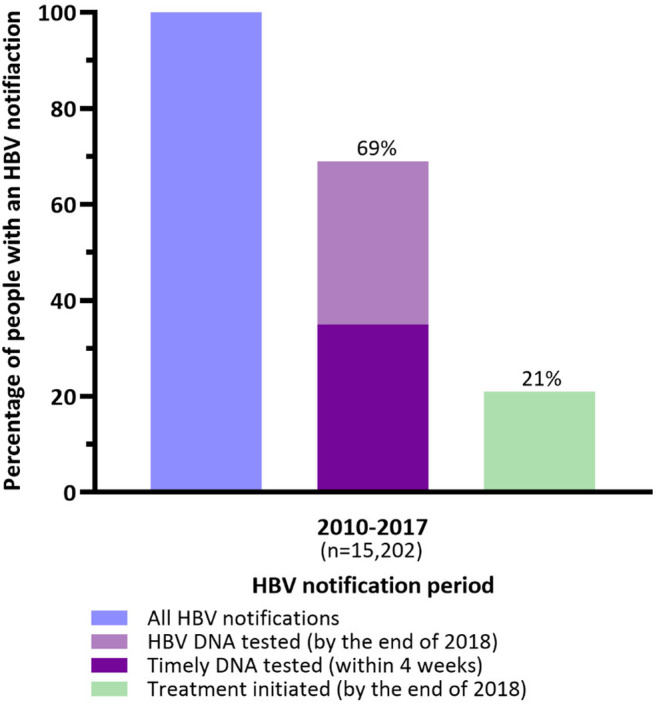
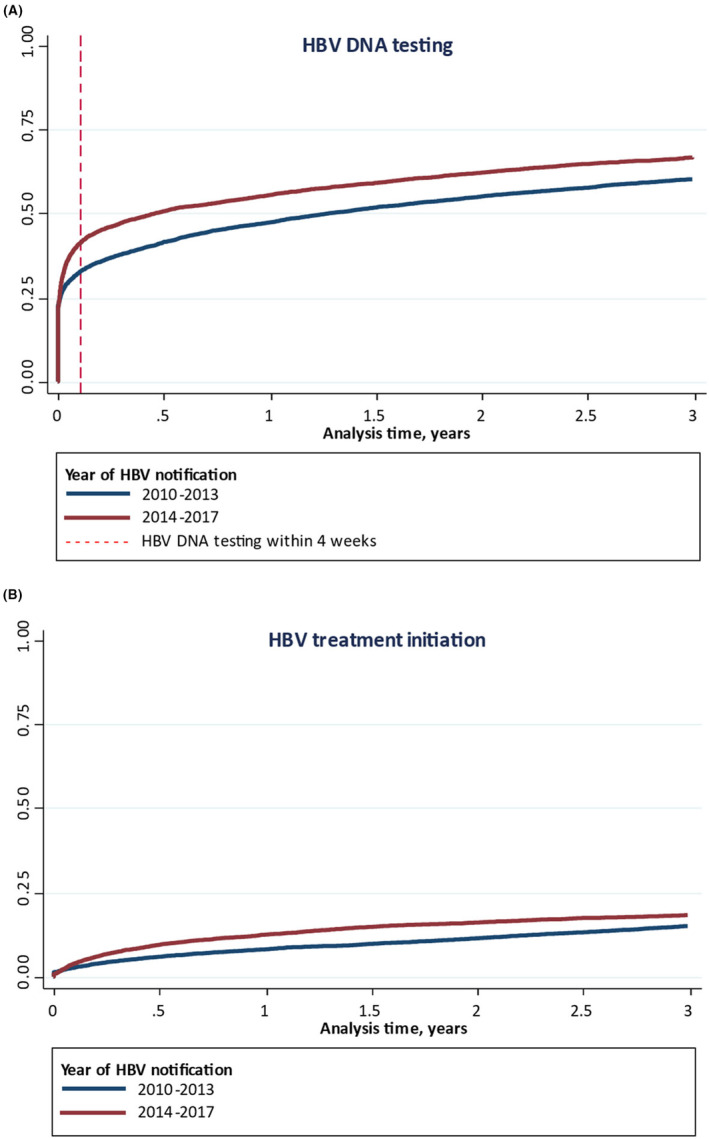
Hepatitis B virus (HBV) care cascade characterisation is important for monitoring HBV elimination progress. This study evaluated care cascade and factors associated with HBV DNA testing and treatment in New South Wales, Australia. HBV care cascade were determined through linkage of HBV notifications (1993-2017) to Medicare and pharmaceutical benefits schemes (2010-2018). Timely HBV DNA testing was within 4 weeks of HBV notification. Multivariate Cox proportional hazards regression evaluated factors associated with HBV DNA testing and treatment. Among 15,202 people with HBV notification, 10,479 (69%) were tested for HBV DNA. A total of 3179 (21%) initiated HBV treatment. HBV DNA testing was more likely among age ≥45 years (adjusted hazard ratio [aHR] 1.07, 95% CI: 1.02, 1.12), hepatocellular carcinoma (HCC) (aHR 1.23, 95% CI: 1.01, 1.50), coinfection (aHR 1.61, 95% CI: 1.23, 2.09), later notification (2014-2017) (aHR 1.21, 95% CI: 1.16, 1.26) and less likely among females (aHR 0.95, 95% CI: 0.91, 0.99), history of alcohol use disorder (AUD) (aHR 0.77, 95% CI: 0.66, 0.89), HCV coinfection (aHR .62, 95% CI: 0.55, 0.70) and Indigenous peoples (aHR 0.84, 95% CI: 0.71, 0.98). HBV treatment was associated with age ≥45 years (aHR 1.35, 95% CI: 1.24, 1.48), decompensated cirrhosis (aHR 2.07, 95% CI: 1.62, 2.65), HCC (aHR 2.96, 95% CI: 2.35, 3.74), HIV coinfection (aHR 4.27, 95% CI: 3.43, 5.31) and later notification (2014-2017) (aHR 1.37, 95% CI: 1.26, 1.47). HBV treatment was less likely among females (aHR 0.68, 95% CI: 0.63, 0.73) and Indigenous peoples (aHR 0.58, 95% CI: 0.42, 0.80). HBV DNA testing and treatment coverage have increased, but remain sub-optimal among some key populations.
乙型肝炎病毒 (HBV) 护理级联特征对于监测 HBV 消除进展非常重要。本研究评估了澳大利亚新南威尔士州 HBV DNA 检测和治疗的护理级联和相关因素。HBV 护理级联是通过将 HBV 通知 (1993-2017 年) 与医疗保险和药品福利计划 (2010-2018 年) 联系起来确定的。及时的 HBV DNA 检测是在 HBV 通知后 4 周内进行的。多变量 Cox 比例风险回归评估了与 HBV DNA 检测和治疗相关的因素。在 15202 名 HBV 通知患者中,有 10479 名 (69%) 接受了 HBV DNA 检测。共有 3179 名 (21%) 开始接受 HBV 治疗。年龄≥45 岁 (调整后的危险比[aHR] 1.07,95%CI:1.02,1.12)、肝细胞癌 (HCC) (aHR 1.23,95%CI:1.01,1.50)、合并感染 (aHR 1.61,95%CI:1.23,2.09)、较晚的通知 (2014-2017 年) (aHR 1.21,95%CI:1.16,1.26) 和女性 (aHR 0.95,95%CI:0.91,0.99)、酒精使用障碍 (AUD) 史 (aHR 0.77,95%CI:0.66,0.89)、HCV 合并感染 (aHR.62,95%CI:0.55,0.70) 和土著人民 (aHR 0.84,95%CI:0.71,0.98) 更有可能进行 HBV DNA 检测。HBV 治疗与年龄≥45 岁 (aHR 1.35,95%CI:1.24,1.48)、失代偿性肝硬化 (aHR 2.07,95%CI:1.62,2.65)、HCC (aHR 2.96,95%CI:2.35,3.74)、HIV 合并感染 (aHR 4.27,95%CI:3.43,5.31) 和较晚的通知 (2014-2017 年) (aHR 1.37,95%CI:1.26,1.47) 相关。女性 (aHR 0.68,95%CI:0.63,0.73) 和土著人民 (aHR 0.58,95%CI:0.42,0.80) 更不可能接受 HBV 治疗。HBV DNA 检测和治疗的覆盖率有所增加,但在一些关键人群中仍不理想。