Giebels Christian, Ehrlich Tristan, Schäfers Hans-Joachim
Department of Thoracic and Cardiovascular Surgery, Saarland University Medical Center, Homburg/Saar, Germany.
Ann Cardiothorac Surg. 2023 Jul 31;12(4):369-376. doi: 10.21037/acs-2023-avs2-12. Epub 2023 Jul 6.
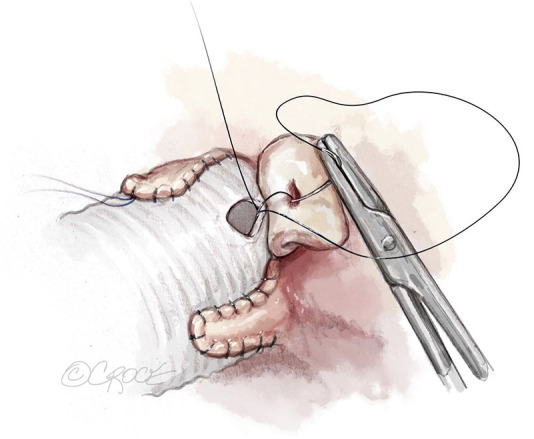
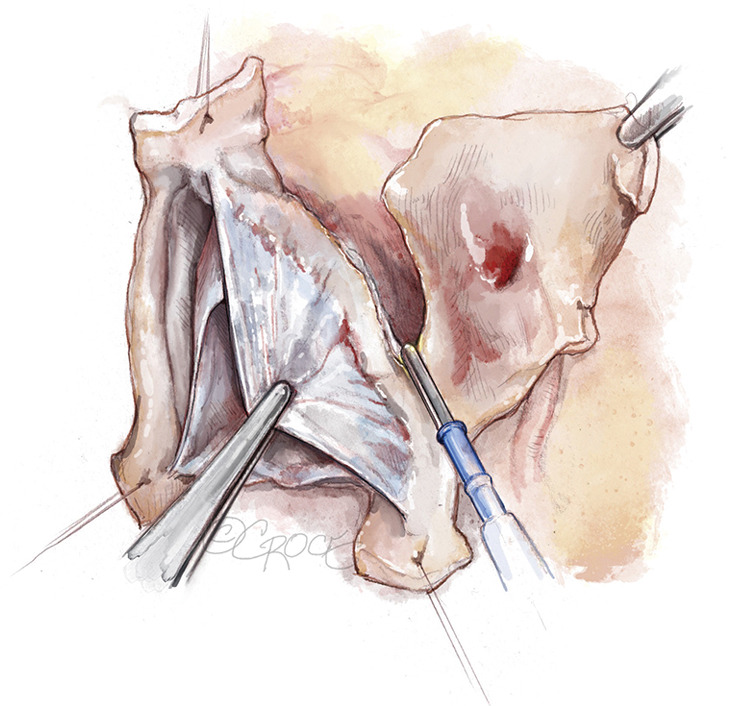
Aortic root remodeling was originally designed in the late 1980s to treat patients with tricuspid aortic valves (TAVs), aortic regurgitation (AR), and root aneurysm to normalize root dimensions. The late results showed a relevant proportion of patients who required reoperation for recurrent AR. Later observations revealed that cusp prolapse is frequently present after correction of root dilatation. We showed that such prolapse could be detected by measuring effective height (eH) and corrected by concomitant cusp repair. In the past 13 years, we have added a suture annuloplasty to improve aortic valve function further. The operation starts with ascertaining adequate cusp size by measuring geometric cusp height. The dilated aortic wall is resected, and a Dacron graft is tailored to create three tongues. These tongues are sutured to the cusp insertion lines. Starting the suture in the nadir allows for easy extension of tongue length to avoid commissural height restriction. A suture annuloplasty is added at nadir level and tied around a Hegar dilator to normalize annular diameter. The valve is assessed visually and by measuring eH. Cusp prolapse (eH <9 mm) is frequent and corrected by free margin plication until all free margins are at equal level and eH is 9 mm. We have employed root remodeling in more than 710 instances of root aneurysm and TAVs. Mean myocardial ischemic time has been 65±13 minutes for isolated remodeling, operative mortality has been 1.5% for elective procedures. With suture annuloplasty, 10-year freedom from reoperation is 95%, even without suture annuloplasty 20-year freedom from reoperation is 85%. In our experience, root remodeling has been a valid form of valve-preserving surgery with low morbidity and mortality and excellent long-term results.
主动脉根部重塑最初设计于20世纪80年代末,用于治疗三尖瓣主动脉瓣(TAV)、主动脉瓣反流(AR)和根部动脉瘤患者,以使根部尺寸正常化。晚期结果显示,有相当一部分患者因复发性AR需要再次手术。后来的观察发现,根部扩张矫正后,瓣叶脱垂经常出现。我们发现,通过测量有效高度(eH)可以检测到这种脱垂,并通过同期瓣叶修复进行矫正。在过去13年中,我们增加了缝合瓣环成形术以进一步改善主动脉瓣功能。手术开始时,通过测量几何瓣叶高度确定瓣叶大小是否合适。切除扩张的主动脉壁,裁剪涤纶补片制成三个舌片。将这些舌片缝合到瓣叶附着线。从最低点开始缝合,便于轻松延长舌片长度,避免瓣交界高度受限。在最低点水平增加缝合瓣环成形术,并围绕海加扩张器打结,以使瓣环直径正常化。通过肉眼和测量eH评估瓣膜。瓣叶脱垂(eH<9mm)很常见,通过游离缘折叠进行矫正,直到所有游离缘处于同一水平且eH为9mm。我们已在710多例根部动脉瘤和TAV病例中采用根部重塑。单纯重塑时,平均心肌缺血时间为65±13分钟,择期手术的手术死亡率为1.5%。采用缝合瓣环成形术时,10年免于再次手术的比例为95%,即使不采用缝合瓣环成形术,20年免于再次手术的比例也为85%。根据我们的经验,根部重塑是一种有效的保留瓣膜手术形式,发病率和死亡率低,长期效果良好。