Division of Population Sciences, Dana-Farber Cancer Institute, Boston, MA; Center for Bioethics, Harvard Medical School, Boston, MA; Division of Hematologic Malignancies, Dana-Farber Cancer Institute, Boston, MA.
Division of Hematologic Malignancies, Dana-Farber Cancer Institute, Boston, MA.
Haematologica. 2024 Apr 1;109(4):1046-1052. doi: 10.3324/haematol.2023.283723.
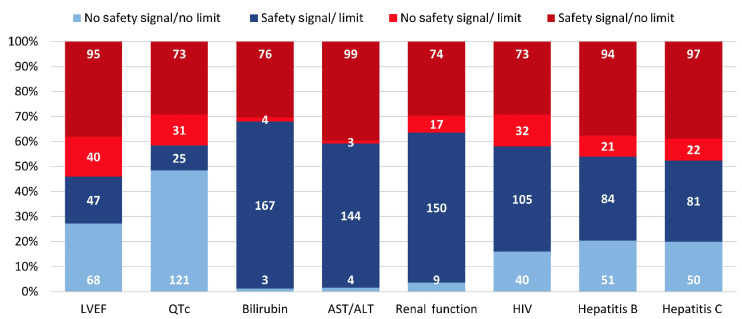
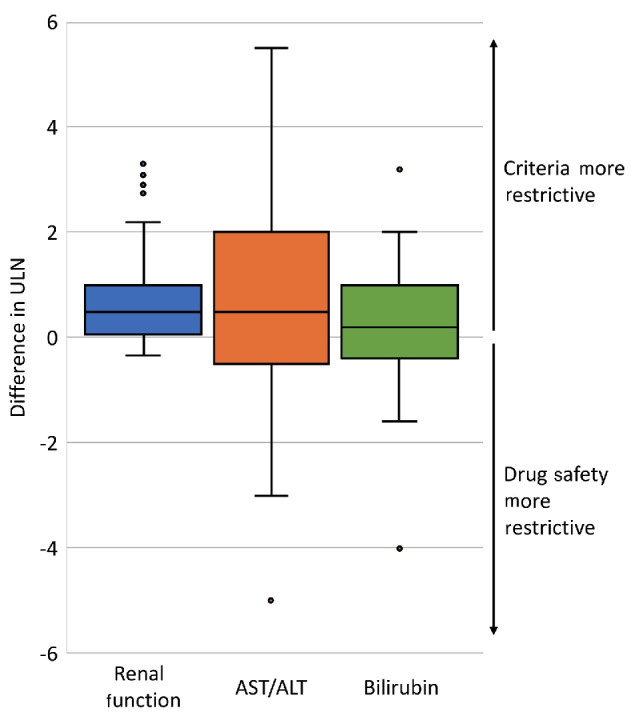
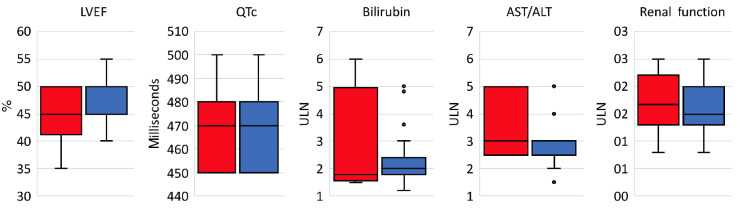
Clinical trial eligibility criteria can unfairly exclude patients or unnecessarily expose them to known risks if criteria are not concordant with drug safety. There are few data evaluating the extent to which acute leukemia eligibility criteria are justified. We analyzed criteria and drug safety data for front-line phase II and/or III acute leukemia trials with start dates 1/1/2010-12/31/2019 registered on clinicaltrials.gov. Multivariable analyses assessed concordance between criteria use and safety data (presence of criteria with a safety signal, or absence of criteria without a signal), and differences between criteria and safety-based limits. Of 250 eligible trials, concordant use of ejection fraction criteria was seen in 34.8%, corrected QT level (QTc) in 22.4%, bilirubin in 68.4%, aspartate transaminase/alanine aminotransferase (AST/ALT) in 58.8%, renal function in 68.4%, human immunodeficiency virus (HIV) in 54.8%, and hepatitis B and C in 42.0% and 41.2%. HIV and hepatitis B and C criteria use was concordant with safety data (adjusted Odds Ratios 2.04 [95%CI: 1.13, 3.66], 2.64 [95%CI: 1.38, 5.04], 2.27 [95%CI: 1.20, 4.32]) but organ function criteria were not (all P>0.05); phase III trials were not more concordant. Bilirubin criteria limits were the same as safety-based limits in 16.0% of trials, AST/ALT in 18.1%, and renal function in 13.9%; in 75.7%, 51.4%, and 56.5% of trials, criteria were more restrictive, respectively, by median differences of 0.2, 0.5, and 0.5 times the upper limits of normal. We found limited drug safety justifications for acute leukemia eligibility criteria. These data define criteria use and limits that can be rationally modified to increase patient inclusion and welfare.
临床试验入选标准如果与药物安全性不一致,可能会不公正地排除患者或不必要地使他们面临已知风险。很少有数据评估急性白血病入选标准的合理性。我们分析了 2010 年 1 月 1 日至 2019 年 12 月 31 日在 clinicaltrials.gov 上注册的一线 II 期和/或 III 期急性白血病试验的入选标准和药物安全性数据。多变量分析评估了标准使用与安全性数据之间的一致性(存在有安全性信号的标准,或不存在无信号的标准),以及标准与基于安全性的限制之间的差异。在 250 项符合条件的试验中,射血分数标准的一致性使用见于 34.8%,校正 QT 水平(QTc)见于 22.4%,胆红素见于 68.4%,天门冬氨酸氨基转移酶/丙氨酸氨基转移酶(AST/ALT)见于 58.8%,肾功能见于 68.4%,人类免疫缺陷病毒(HIV)见于 54.8%,乙型肝炎和丙型肝炎分别见于 42.0%和 41.2%。HIV 和乙型肝炎、丙型肝炎入选标准与安全性数据一致(调整后的优势比为 2.04[95%置信区间:1.13,3.66]、2.64[95%置信区间:1.38,5.04]、2.27[95%置信区间:1.20,4.32]),但器官功能标准不一致(均 P>0.05);III 期试验没有更一致。16.0%的试验中胆红素标准的界限与基于安全性的界限相同,AST/ALT 为 18.1%,肾功能为 13.9%;在 75.7%、51.4%和 56.5%的试验中,标准分别分别通过中位数差异为 0.2、0.5 和 0.5 倍正常上限更具限制性。我们发现急性白血病入选标准的药物安全性理由有限。这些数据定义了可以合理修改的标准使用和限制,以增加患者纳入和福利。