Aberdeen Centre for Health Data Science, School of Medicine, Medical Sciences and Nutrition, University of Aberdeen, Aberdeen, UK.
Department of Renal Medicine, NHS Grampian, Aberdeen, UK.
Nephrol Dial Transplant. 2024 Feb 28;39(3):426-435. doi: 10.1093/ndt/gfad180.
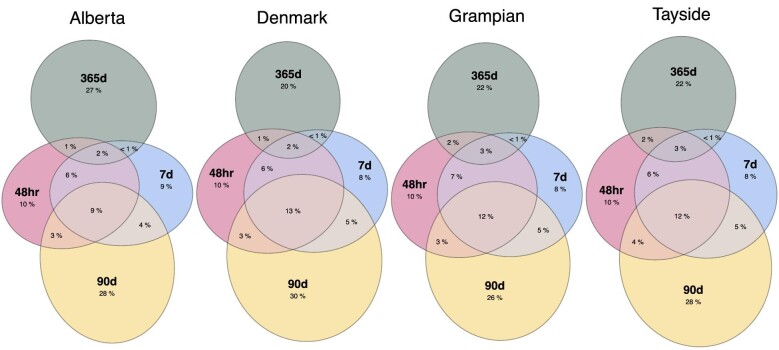
There are no consensus definitions for evaluating kidney function recovery after acute kidney injury (AKI) and acute kidney disease (AKD), nor is it clear how recovery varies across populations and clinical subsets. We present a federated analysis of four population-based cohorts from Canada, Denmark and Scotland, 2011-18.
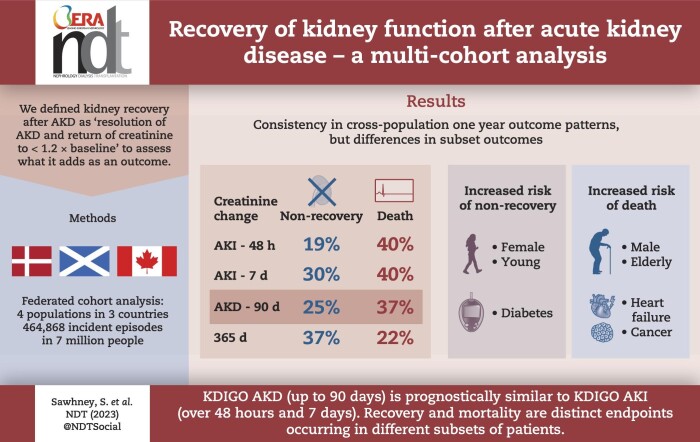
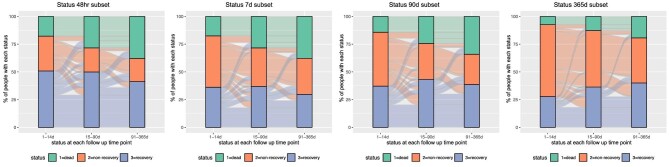
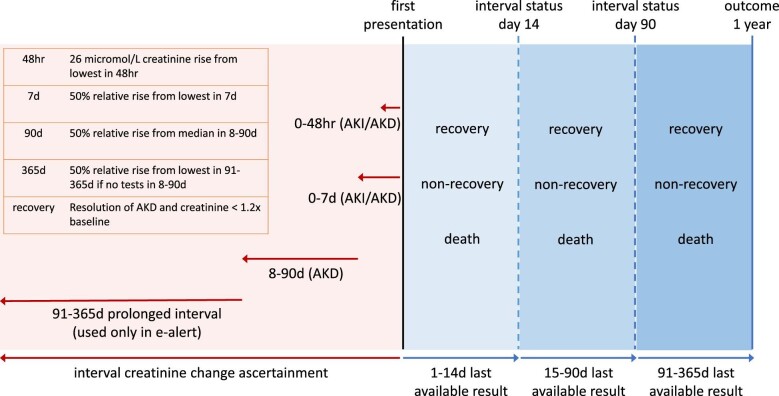
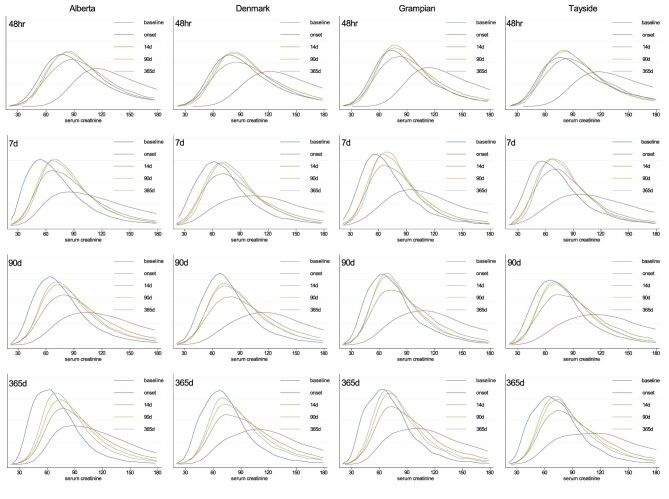
We identified incident AKD defined by serum creatinine changes within 48 h, 7 days and 90 days based on KDIGO AKI and AKD criteria. Separately, we applied changes up to 365 days to address widely used e-alert implementations that extend beyond the KDIGO AKI and AKD timeframes. Kidney recovery was based on resolution of AKD and a subsequent creatinine measurement below 1.2× baseline. We evaluated transitions between non-recovery, recovery and death up to 1 year; within age, sex and comorbidity subgroups; between subset AKD definitions; and across cohorts.
There were 464 868 incident cases, median age 67-75 years. At 1 year, results were consistent across cohorts, with pooled mortalities for creatinine changes within 48 h, 7 days, 90 days and 365 days (and 95% confidence interval) of 40% (34%-45%), 40% (34%-46%), 37% (31%-42%) and 22% (16%-29%) respectively, and non-recovery of kidney function of 19% (15%-23%), 30% (24%-35%), 25% (21%-29%) and 37% (30%-43%), respectively. Recovery by 14 and 90 days was frequently not sustained at 1 year. Older males and those with heart failure or cancer were more likely to die than to experience sustained non-recovery, whereas the converse was true for younger females and those with diabetes.
Consistently across multiple cohorts, based on 1-year mortality and non-recovery, KDIGO AKD (up to 90 days) is at least prognostically similar to KDIGO AKI (7 days), and covers more people. Outcomes associated with AKD vary by age, sex and comorbidities such that older males are more likely to die, and younger females are less likely to recover.
目前,尚无评估急性肾损伤(AKI)和急性肾疾病(AKD)后肾功能恢复的共识定义,也不清楚人群和临床亚组之间的恢复情况有何不同。我们呈现了一项来自加拿大、丹麦和苏格兰的四个基于人群的队列的联邦分析,时间范围为 2011 年至 2018 年。
我们根据 KDIGO AKI 和 AKD 标准,在 48 小时、7 天和 90 天内基于血清肌酐变化确定了新发生的 AKD。此外,我们还应用了 365 天内的变化来解决广泛使用的 e-alert 实施情况,这些实施情况超出了 KDIGO AKI 和 AKD 的时间范围。肾脏恢复是基于 AKD 的解决和随后的肌酐测量值低于 1.2×基线。我们评估了 1 年内非恢复、恢复和死亡之间的转变;在年龄、性别和合并症亚组内;在亚组 AKD 定义之间;以及在队列之间。
共纳入了 464868 例新发病例,中位年龄为 67-75 岁。1 年后,结果在各个队列中是一致的,在 48 小时、7 天、90 天和 365 天内肌酐变化的 pooled 死亡率(95%置信区间)分别为 40%(34%-45%)、40%(34%-46%)、37%(31%-42%)和 22%(16%-29%),肾功能无恢复的比例分别为 19%(15%-23%)、30%(24%-35%)、25%(21%-29%)和 37%(30%-43%)。14 天和 90 天的恢复在 1 年内通常不能持续。年龄较大的男性和患有心力衰竭或癌症的患者比持续无恢复更有可能死亡,而年龄较小的女性和患有糖尿病的患者则相反。
基于 1 年死亡率和无恢复情况,多个队列中 KDIGO AKD(最长至 90 天)至少在预后方面与 KDIGO AKI(7 天)相似,并且涵盖了更多的人群。AKD 相关结局因年龄、性别和合并症而异,年龄较大的男性更有可能死亡,年龄较小的女性更不可能恢复。