Division of Cardiac Critical Care Medicine, Department of Anesthesiology and Critical Care, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States.
Division of Cardiology, Department of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States.
Resuscitation. 2023 Oct;191:109936. doi: 10.1016/j.resuscitation.2023.109936. Epub 2023 Aug 11.
Global longitudinal strain (GLS) is an echocardiographic method to identify left ventricular (LV) dysfunction after cardiac arrest that is less sensitive to loading conditions. We aimed to identify the frequency of impaired GLS following pediatric cardiac arrest, and its association with hospital mortality.
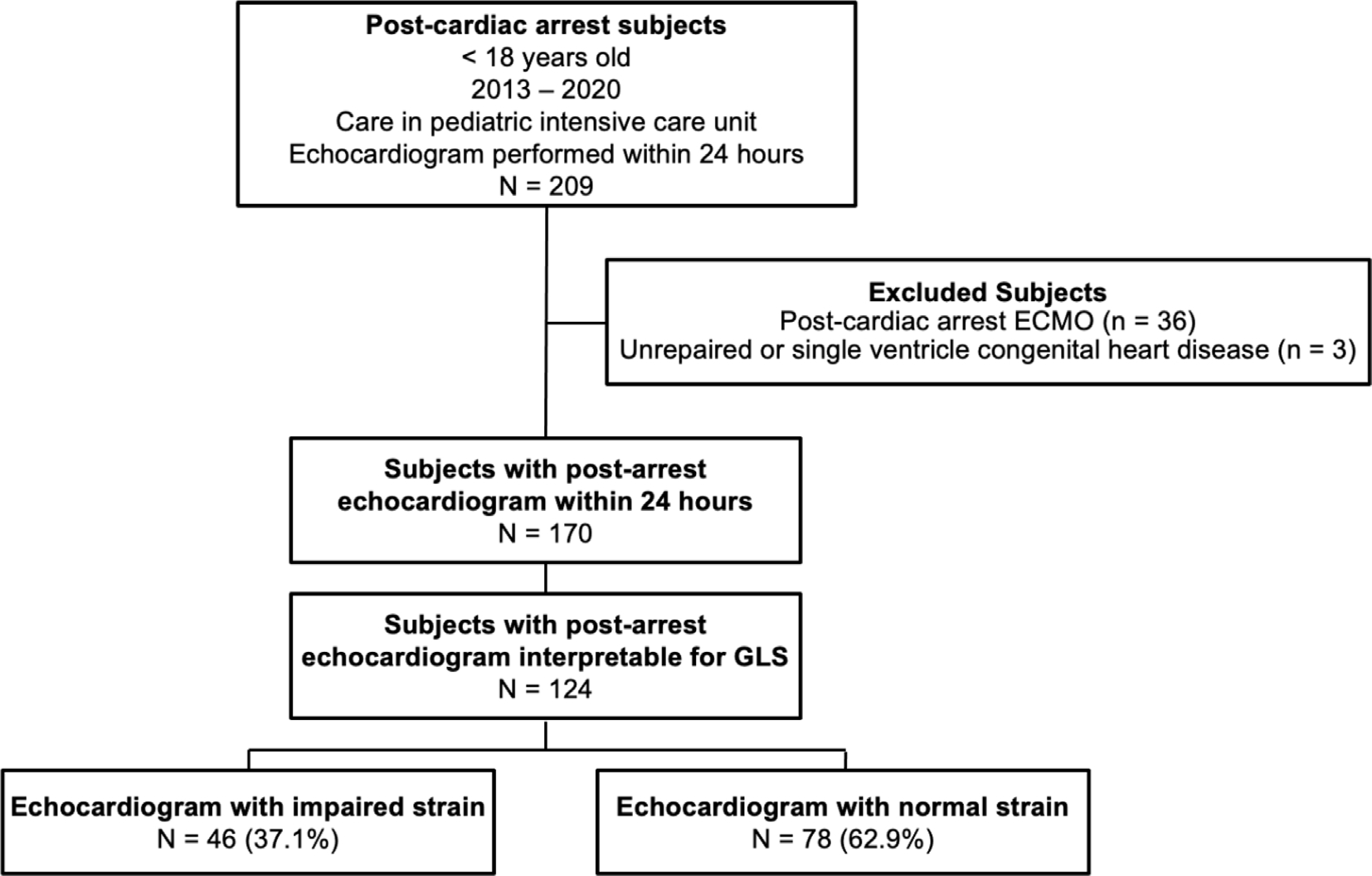
This is a retrospective single-center cohort study of children <18 years of age treated in the pediatric intensive care unit (PICU) after in- or out-of-hospital cardiac arrest (IHCA and OHCA), with echocardiogram performed within 24 hours of initiation of post-arrest PICU care between 2013 and 2020. Patients with congenital heart disease, post-arrest extracorporeal support, or inability to measure GLS were excluded. Echocardiographic LV ejection fraction (EF) and shortening fraction (SF) were abstracted from the chart. GLS was measured post hoc; impaired strain was defined as LV GLS ≥ 2 SD worse than age-dependent normative values. Demographics and pre-arrest, arrest, and post-arrest characteristics were compared between subjects with normal versus impaired GLS. Correlation between GLS, SF and EF were calculated with Pearson comparison. Logistic regression tested the association of GLS with mortality. Area under the receiver operator curve (AUROC) was calculated for discriminative utility of GLS, EF, and SF with mortality.
GLS was measured in 124 subjects; impaired GLS was present in 46 (37.1%). Subjects with impaired GLS were older (median 7.9 vs. 1.9 years, p < 0.001), more likely to have ventricular tachycardia/fibrillation as initial rhythm (19.6% versus 3.8%, p = 0.017) and had higher peak troponin levels in the first 24 hours post-arrest (median 2.5 vs. 0.5, p = 0.002). There were no differences between arrest location or CPR duration by GLS groups. Subjects with impaired GLS compared to normal GLS had lower median EF (42.6% versus 62.3%) and median SF (23.3% versus 36.6%), all p < 0.001, with strong inverse correlation between GLS and EF (rho -0.76, p < 0.001) and SF (rho -0.71, p < 0.001). Patients with impaired GLS had higher rates of mortality (60% vs. 32%, p = 0.009). GLS was associated with mortality when controlling for age and initial rhythm [aOR 1.17 per 1% increase in GLS (95% CI 1.09-1.26), p < 0.001]. GLS, EF and SF had similar discrimination for mortality: GLS AUROC 0.69 (95% CI 0.60-0.79); EF AUROC 0.71 (95% CI 0.58-0.88); SF AUROC 0.71 (95% CI 0.61-0.82), p = 0.101.
Impaired LV function as measured by GLS after pediatric cardiac arrest is associated with hospital mortality. GLS is a novel complementary metric to traditional post-arrest echocardiography that correlates strongly with EF and SF and is associated with mortality. Future large prospective studies of post-cardiac arrest care should investigate the prognostic utilities of GLS, alongside SF and EF.
全球纵向应变(GLS)是一种超声心动图方法,可用于识别心脏骤停后的左心室(LV)功能障碍,其对负荷条件的敏感性较低。我们旨在确定儿科心脏骤停后 GLS 受损的频率及其与住院死亡率的关系。
这是一项回顾性的单中心队列研究,纳入了在 2013 年至 2020 年期间于儿科重症监护病房(PICU)接受治疗的年龄<18 岁的儿童,这些儿童在心脏骤停后 PICU 治疗开始后 24 小时内行超声心动图检查,包括院内和院外心脏骤停(IHCA 和 OHCA)。排除了患有先天性心脏病、心脏骤停后体外支持或无法测量 GLS 的患者。从图表中提取超声心动图左心室射血分数(EF)和缩短分数(SF)。GLS 是事后测量的;受损的应变定义为 LV GLS 比年龄依赖性正常参考值差≥2 个标准差。比较正常 GLS 和受损 GLS 受试者的一般资料以及发病前、发病时和发病后的特征。使用 Pearson 比较计算 GLS 与 SF 和 EF 之间的相关性。Logistic 回归测试 GLS 与死亡率的关系。计算 GLS、EF 和 SF 与死亡率的受试者工作特征曲线(ROC)下面积(AUROC)以评估其对死亡率的区分能力。
在 124 名受试者中测量了 GLS;其中 46 名(37.1%)存在受损的 GLS。与 GLS 正常的受试者相比,GLS 受损的受试者年龄更大(中位数 7.9 岁 vs. 1.9 岁,p<0.001),初始节律更可能为室性心动过速/颤动(19.6% vs. 3.8%,p=0.017),并且在心脏骤停后 24 小时内的峰值肌钙蛋白水平更高(中位数 2.5 与 0.5,p=0.002)。两组之间的发病位置或心肺复苏持续时间没有差异。与 GLS 正常的受试者相比,GLS 受损的受试者的中位 EF(42.6% vs. 62.3%)和中位 SF(23.3% vs. 36.6%)更低,所有 p 值均<0.001,GLS 与 EF(rho -0.76,p<0.001)和 SF(rho -0.71,p<0.001)呈强负相关。GLS 受损的患者死亡率更高(60% vs. 32%,p=0.009)。在校正年龄和初始节律后,GLS 与死亡率相关[aOR 每增加 1% GLS 则死亡率增加 1.17(95%CI 1.09-1.26),p<0.001]。GLS、EF 和 SF 对死亡率的区分能力相似:GLS AUROC 为 0.69(95%CI 0.60-0.79);EF AUROC 为 0.71(95%CI 0.58-0.88);SF AUROC 为 0.71(95%CI 0.61-0.82),p=0.101。
儿科心脏骤停后左心室功能受损,由 GLS 测量,与住院死亡率相关。GLS 是一种新的补充性心脏骤停后超声心动图指标,与 EF 和 SF 相关性强,与死亡率相关。未来关于心脏骤停后护理的大型前瞻性研究应探讨 GLS 与 SF 和 EF 一起的预后效用。