Cardiac Surgery Unit, Cardio-Thoracic Department, University of Brescia, Brescia, Italy.
Center for Neuroscience, Queen's University, Kingston, Ontario, Canada.
J Cardiovasc Med (Hagerstown). 2024 Jan 1;25(1):30-37. doi: 10.2459/JCM.0000000000001544. Epub 2023 Aug 2.
Timing and surgical strategies in acute infective endocarditis are still questionable. We sought to investigate clinical outcomes of patients undergoing mitral valve repair (MVR) compared with mitral valve replacement [mitral valve prosthesis (MVP)] for acute infective endocarditis.
From 2004 to 2019, 109 consecutive patients with acute mitral valve infective endocarditis were retrospectively investigated. Patients were divided into two groups according to surgical strategy: MVR 53/109 (48.6%) versus MVP 56/109 (51.4%). Primary end points were in-hospital mortality and overall survival at 10 years. Secondary end point was the freedom from infective endocarditis relapse.
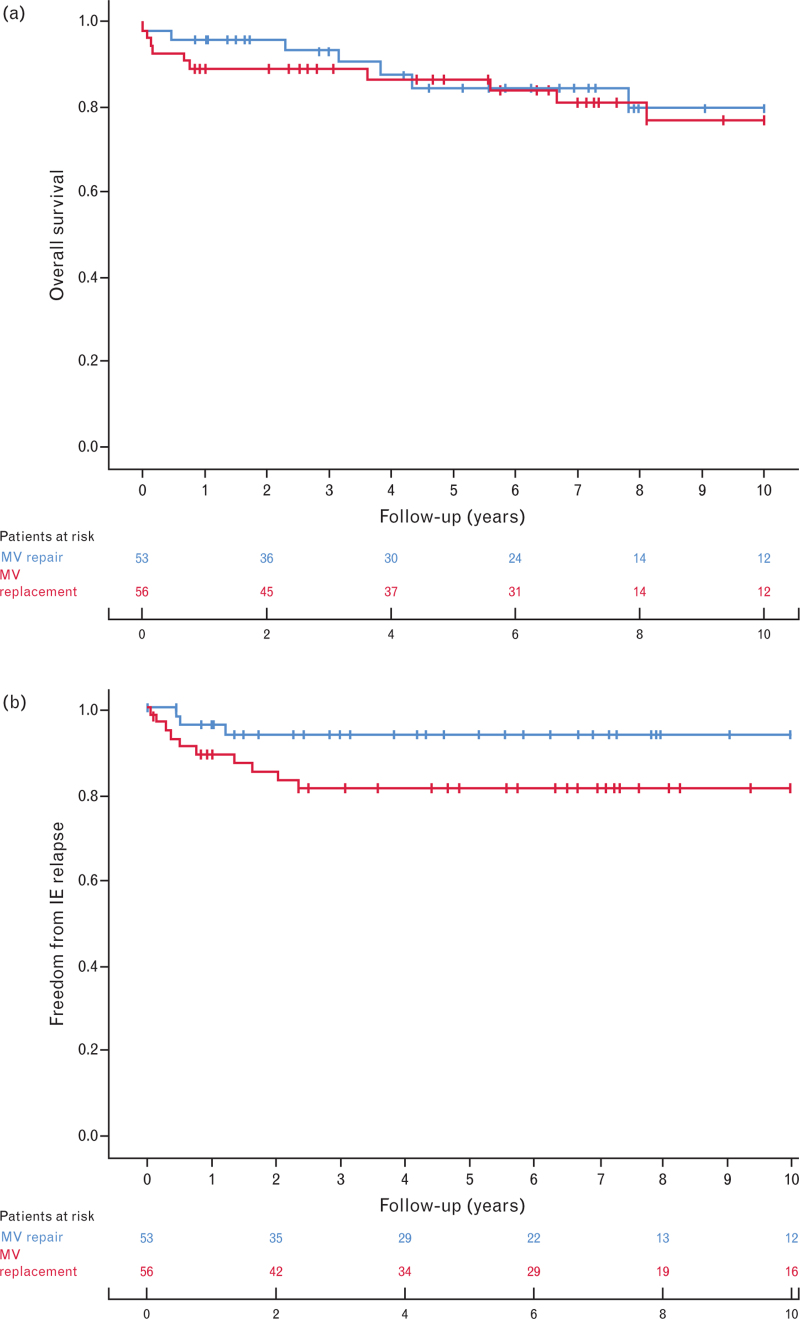
Our institutional surgical approach for infective endocarditis allowed us to achieve MVR in 48.6% of patients. Hospital mortality was comparable between the two groups [MVR: 1/53 (1.9%) versus MVP: 2/56 (3.6%), P = 1.000]. Overall 10-year survival was 80.0 ± 14.1 and 77.2 ± 13.5% for MVR and MVP, respectively ( P = 0.648). MVR showed a lower incidence of infective endocarditis relapse compared with MVP (MVR: 93.6 ± 7.1 versus MVP: 80.9 ± 10.8%, P = 0.041). At Cox regression, infective endocarditis relapse was an independent risk factor for death (hazard ratio 4.03; 95% confidence interval 1.41-11.52; P = 0.009).
The tendency to postpone surgery in stable patients with mitral infective endocarditis allowed achievement of MVR in almost 50% of patients. Although repair remains the approach of choice in our institution, no differences between MVR and MVP were reported in terms of early/late survival. However, MVP had a higher incidence of infective endocarditis relapse that represents an independent risk of mortality.
急性感染性心内膜炎的时机和手术策略仍存在争议。我们旨在研究接受二尖瓣修复术(MVR)与二尖瓣置换术(MVP)治疗急性感染性心内膜炎的患者的临床结局。
从 2004 年至 2019 年,回顾性调查了 109 例连续的急性二尖瓣感染性心内膜炎患者。根据手术策略将患者分为两组:MVR 53/109(48.6%)与 MVP 56/109(51.4%)。主要终点是住院死亡率和 10 年总生存率。次要终点是无感染性心内膜炎复发的生存率。
我们的机构感染性心内膜炎手术方法使我们能够在 48.6%的患者中实现 MVR。两组的住院死亡率相当[MVR:1/53(1.9%)与 MVP:2/56(3.6%),P=1.000]。总体 10 年生存率分别为 MVR:80.0±14.1%和 MVP:77.2±13.5%(P=0.648)。MVR 的感染性心内膜炎复发发生率低于 MVP(MVR:93.6±7.1 与 MVP:80.9±10.8%,P=0.041)。Cox 回归分析显示,感染性心内膜炎复发是死亡的独立危险因素(危险比 4.03;95%置信区间 1.41-11.52;P=0.009)。
在稳定的二尖瓣感染性心内膜炎患者中,手术推迟的倾向使近 50%的患者能够实现 MVR。尽管修复仍然是我们机构的首选方法,但 MVR 和 MVP 在早期/晚期生存率方面没有差异。然而,MVP 的感染性心内膜炎复发发生率较高,这是死亡的独立危险因素。