Mikus Elisa, Fiorentino Mariafrancesca, Sangiorgi Diego, Pascale Renato, Costantino Antonino, Nocera Chiara, Calvi Simone, Tenti Elena, Tremoli Elena, Tripodi Alberto, Savini Carlo
Cardiovascular Department, Maria Cecilia Hospital, GVM Care & Research, 48033 Cotignola, Ravenna, Italy.
Department of Medical and Surgical Sciences, Alma Mater Studiorum University of Bologna, 40138 Bologna, Italy.
Microorganisms. 2024 Jun 28;12(7):1320. doi: 10.3390/microorganisms12071320.
The benefits of mitral repair versus replacement for endocarditis are inconclusive. This study compares outcomes of patients with infective endocarditis undergoing mitral valve repair versus replacement and investigates the impact of microbial etiology.
All 251 patients undergoing mitral valve surgery for active endocarditis between 2010 and 2023 were enrolled, 180 (71.7%) replacement and 71 (28.3%) repair. To adjust for imbalances, inverse probability of treatment weighting was applied and 187 patients were obtained.
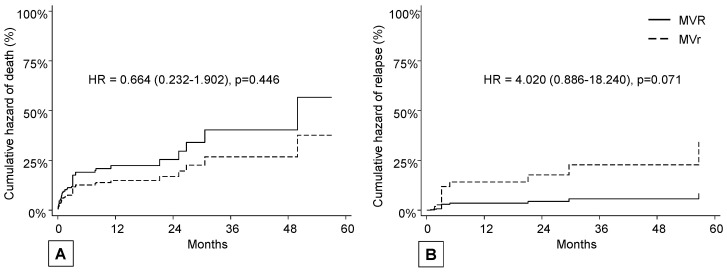
The analysis between groups, following the application of inverse probability of treatment weighting, showed no statistically significant differences across all considered outcomes. Early and late death was observed respectively in 6 (8.5%) and 11 (15.5%) patients in the repair group versus 24 (13.3%) and 45 (25.0%) in the replacement group without statistical significance ( = 0.221 and = 0.446). Relapse occurred in six patients (8.5%) in the repair group after a median time of 4.0 months and in six (3.3%) in the replacement after 6.9 months ( = 0.071).
Surgical strategy in mitral endocarditis has no effect on major postoperative complications, mortality, or medium/long-term survival. and represent a risk for early mortality and relapse. However, mitral valve repair for endocarditis can be pursued when it ensures the complete eradication of all infected tissue, particularly in cases caused by infection, in young patients, and after a minimum of 18 days of antibiotic therapy.
二尖瓣修复术与置换术治疗心内膜炎的益处尚无定论。本研究比较了感染性心内膜炎患者接受二尖瓣修复术与置换术的结果,并调查了微生物病因的影响。
纳入2010年至2023年间因活动性心内膜炎接受二尖瓣手术的所有251例患者,其中180例(71.7%)接受置换术,71例(28.3%)接受修复术。为了调整不均衡性,应用治疗权重的逆概率,最终获得187例患者。
在应用治疗权重的逆概率后,组间分析显示,在所有考虑的结果中均无统计学显著差异。修复组分别有6例(8.5%)和11例(15.5%)患者发生早期和晚期死亡,置换组分别为24例(13.3%)和45例(25.0%),无统计学显著性(P = 0.221和P = 0.446)。修复组6例患者(8.5%)在中位时间4.0个月后复发,置换组6例患者(3.3%)在6.9个月后复发(P = 0.071)。
二尖瓣心内膜炎的手术策略对术后主要并发症、死亡率或中长期生存无影响。[具体微生物名称1]和[具体微生物名称2]是早期死亡和复发的危险因素。然而,当二尖瓣修复术能确保彻底清除所有感染组织时,可采用该术式,特别是在由[具体微生物名称1]感染引起的病例、年轻患者以及至少18天抗生素治疗后。