Grisham Rachel N, Vergote Ignace, Banerjee Susana, Drill Esther, Kalbacher Elsa, Mirza Mansoor Raza, Romero Ignacio, Vuylsteke Peter, Coleman Robert L, Hilpert Felix, Oza Amit M, Westermann Anneke, Oehler Martin K, Pignata Sandro, Aghajanian Carol, Colombo Nicoletta, Cibula David, Moore Kathleen N, Del Campo Josep M, Berger Regina, Marth Christian, Sehouli Jalid, O'Malley David M, Churruca Cristina, Kristensen Gunnar, Clamp Andrew, Farley John, Iyer Gopa, Ray-Coquard Isabelle, Monk Bradley J
Memorial Sloan Kettering Cancer Center, Weill Cornell Medical Center, New York, New York.
Belgium and Luxemburg Gynaecological Oncology Group, University Hospitals Leuven, Leuven, Belgium.
Clin Cancer Res. 2023 Oct 13;29(20):4068-4075. doi: 10.1158/1078-0432.CCR-23-0621.
We present the results of a post hoc tumor tissue analysis from the phase 3 MILO/ENGOT-ov11 study (NCT01849874).
Mutation/copy-number analysis was performed on tissue obtained pre-randomization. The Kaplan-Meier method was used to estimate progression-free survival (PFS). Unbiased univariate analysis, Cox regression, and binary logistic regression were used to test associations between mutation status and outcomes, including PFS and binary response by local RECIST 1.1.
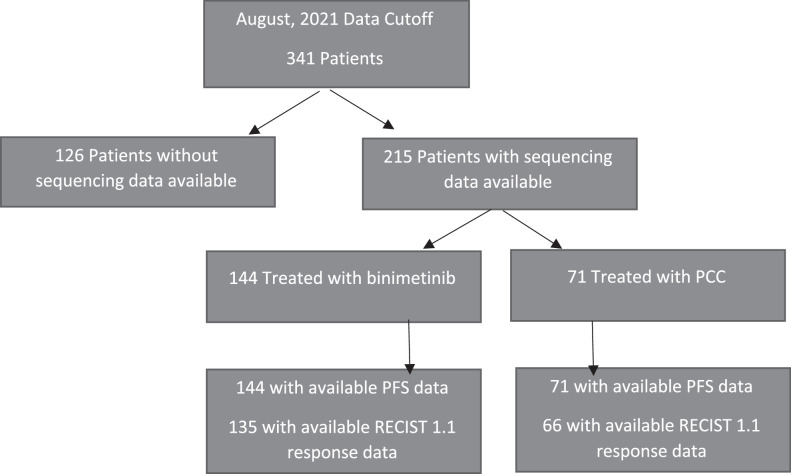
MILO/ENGOT-ov11 enrolled 341 patients, ranging in age from 22 to 79, from June, 2013 to April, 2016. Patients were randomized 2:1 to binimetinib or physician's choice of chemotherapy (PCC). The most commonly altered gene was KRAS (33%). In 135 patients treated with binimetinib with response rate (RR) data, other detected MAPK pathway alterations included: NRAS (n = 11, 8.1%), BRAF V600E (n = 8, 5.9%), RAF1 (n = 2, 1.5%), and NF1 (n = 7, 5.2%). In those with and without MAPK pathway alterations, the RRs with binimetinib were 41% and 13%, respectively. PFS was significantly longer in patients with, compared with those without, MAPK pathway alterations treated with binimetinib [HR, 0.5; 95% confidence interval (CI) 0.31-0.79]. There was a nonsignificant trend toward PFS improvement in PCC-treated patients with MAPK pathway alterations compared with those without (HR, 0.82; 95% CI, 0.43-1.59).
Although this hypothesis-generating analysis is limited by multiple testing, higher RRs and longer PFS were seen in patients with low-grade serous ovarian cancer (LGSOC) treated with binimetinib, and to a lesser extent in those treated with PCC, who harbored MAPK pathway alterations. Somatic tumor testing should be routinely considered in patients with LGSOC and used as a future stratification factor.
我们展示了3期MILO/ENGOT-ov11研究(NCT01849874)的事后肿瘤组织分析结果。
对随机分组前获取的组织进行突变/拷贝数分析。采用Kaplan-Meier法评估无进展生存期(PFS)。使用无偏单因素分析、Cox回归和二元逻辑回归来检验突变状态与结局之间的关联,包括PFS和根据局部RECIST 1.1标准的二元反应。
2013年6月至2016年4月期间,MILO/ENGOT-ov11研究共纳入341例年龄在22岁至79岁之间的患者。患者按2:1随机分配接受比美替尼或医生选择的化疗(PCC)。最常发生改变的基因是KRAS(33%)。在135例有缓解率(RR)数据的接受比美替尼治疗的患者中,其他检测到的MAPK通路改变包括:NRAS(n = 11,8.1%)、BRAF V600E(n = 8,5.9%)、RAF1(n = 2,1.5%)和NF1(n = 7,5.2%)。在有和没有MAPK通路改变的患者中,接受比美替尼治疗的RR分别为41%和13%。接受比美替尼治疗的有MAPK通路改变的患者的PFS显著长于无该通路改变的患者[风险比(HR),0.5;95%置信区间(CI)0.31 - 0.79]。与无MAPK通路改变的PCC治疗患者相比,有该通路改变的患者在PFS改善方面有不显著的趋势(HR,0.82;95% CI,0.43 - 1.59)。
尽管这项产生假设的分析受到多重检验的限制,但在接受比美替尼治疗的低级别浆液性卵巢癌(LGSOC)患者中观察到了更高的RR和更长的PFS,在接受PCC治疗且存在MAPK通路改变的患者中程度较轻。对于LGSOC患者应常规考虑进行体细胞肿瘤检测,并将其用作未来的分层因素。